ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Key Takeaways
- Performance anxiety triggers compensatory hypervigilance that temporarily masks ADHD symptoms but depletes mental
- Chronic anxiety leads to exhaustion and burnout, creating conditions for depression to emerge
- Depression further impairs executive function, worsening the ADHD symptoms that initiated the cycle
- Depressive withdrawal reduces structure and routine, which individuals with ADHD particularly need to function optimally
- The worsened ADHD symptoms create new failures, restarting the anxiety cycle
The relationship between ADHD and mood disorders is far more intricate than simple co-occurrence. When ADHD appears alongside anxiety and depression, these conditions often create reinforcing cycles that can intensify symptoms and complicate both diagnosis and management. Research suggests that adults with ADHD experience comorbid anxiety disorders at rates substantially higher than the general population, while depression frequently emerges as a secondary response to chronic stress and functional impairment. Understanding how these conditions interact—and particularly how anxiety and depression can feed into one another in the context of ADHD—is essential for developing effective coping strategies and seeking appropriate support.
This article examines the mechanisms behind ADHD comorbidity with anxiety and depression cycles, explores why these patterns develop, and offers evidence-based approaches for breaking the cycle and managing all three conditions simultaneously.
ADHD is fundamentally a neurodevelopmental condition characterized by differences in executive function, attention regulation, and impulse control. These differences stem from variations in brain structure and neurochemical functioning, particularly involving dopamine and norepinephrine systems. What makes ADHD particularly vulnerable to comorbidity is that the same neural systems implicated in attention and executive function also play significant roles in emotional regulation and stress response.
Research from major academic institutions suggests that individuals with ADHD often experience heightened emotional reactivity and difficulty modulating emotional responses. This isn't simply a behavioral issue—it reflects actual differences in how the brain processes and regulates emotional information. When executive function deficits impair someone's ability to plan, organize, and follow through on tasks, the resulting life experiences create fertile ground for anxiety and depression to develop.
The prefrontal cortex, which is central to both executive function and emotional regulation, shows altered patterns of activation in ADHD. This same brain region is implicated in depression and anxiety disorders, creating overlapping vulnerabilities. When someone with ADHD faces repeated experiences of underperformance, missed deadlines, or social difficulties, these experiences can trigger anxious hypervigilance about future failures and depressive responses to perceived inadequacy.
Understanding this neurobiological foundation helps explain why ADHD comorbidity with anxiety and depression isn't simply bad luck—it's a predictable outcome of how these conditions interact at the level of brain function and lived experience.
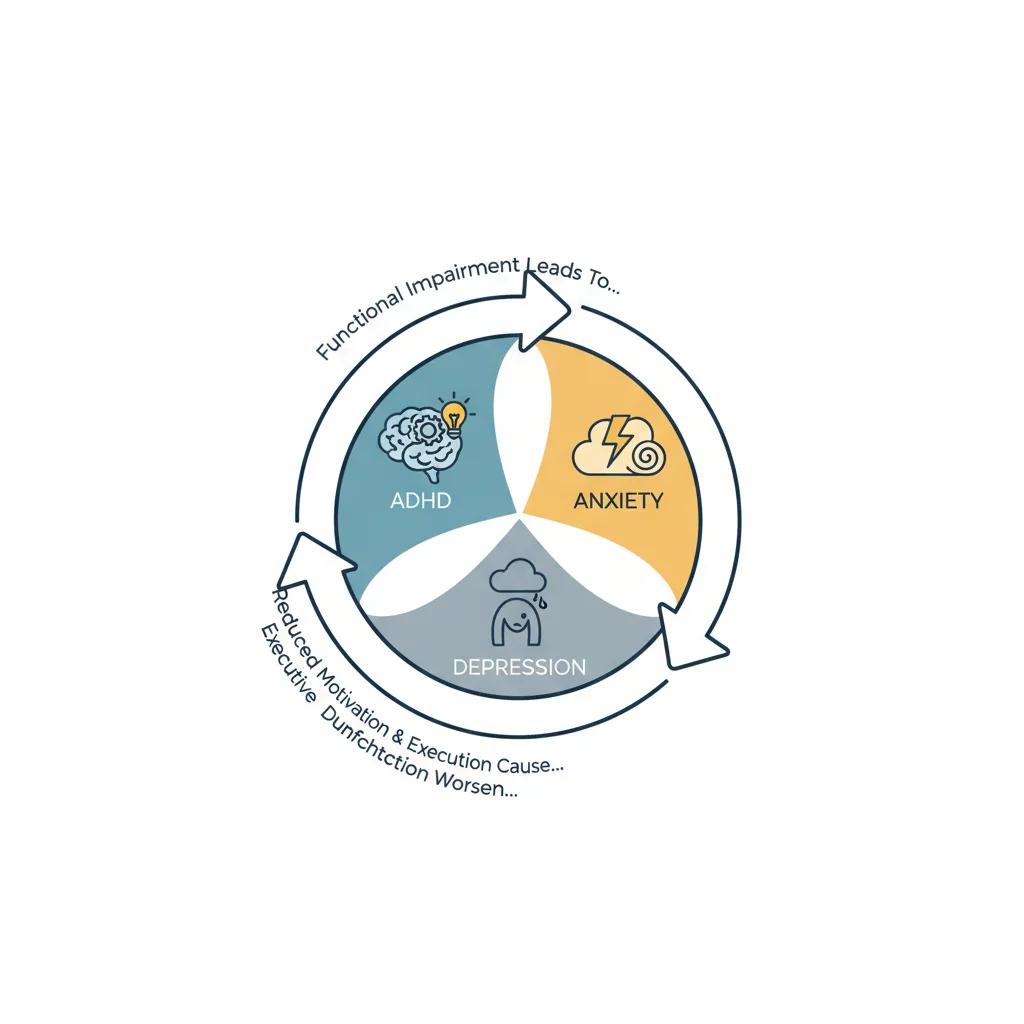
The cycle between anxiety and depression in individuals with ADHD often follows a recognizable pattern, though the specific manifestation varies between individuals. Typically, the cycle begins with ADHD-related functional impairments: difficulty completing work tasks, forgetting important commitments, struggling with time management, or underperforming relative to one's abilities.
These difficulties generate anxiety—worry about upcoming deadlines, fear of negative evaluation, hypervigilance about potential mistakes. In the short term, anxiety might even appear to "help" by creating urgency that temporarily compensates for ADHD-related procrastination. However, anxiety also consumes cognitive resources, worsens concentration, disrupts sleep, and increases overall stress burden.
Key elements of the anxiety-depression cycle in ADHD:
- Performance anxiety triggers compensatory hypervigilance that temporarily masks ADHD symptoms but depletes mental resources
- Chronic anxiety leads to exhaustion and burnout, creating conditions for depression to emerge
- Depression further impairs executive function, worsening the ADHD symptoms that initiated the cycle
- Depressive withdrawal reduces structure and routine, which individuals with ADHD particularly need to function optimally
- The worsened ADHD symptoms create new failures, restarting the anxiety cycle
As depression develops, motivation declines, cognitive processing slows, and the executive function challenges inherent to ADHD become even more pronounced. Tasks that were merely difficult become overwhelming. The person withdraws from activities, relationships suffer, and daily structure deteriorates. This deterioration creates new sources of anxiety—concern about declined performance, worry about damaged relationships, fear about the future.
Eventually, either the anxiety reaches a crisis point that forces action, or external deadlines create unavoidable pressure. The person mobilizes again, driven by anxiety, and the cycle repeats. Each repetition can deepen the groove, making the pattern more automatic and harder to interrupt.
One of the most significant challenges in addressing cyclical patterns of depression anxiety in ADHD patients is accurate diagnosis. The symptoms of these conditions overlap substantially, and each can mask or mimic the others. Inattention, for instance, is a hallmark of ADHD but also appears prominently in depression and anxiety disorders. Difficulty with decision-making occurs in all three conditions. Irritability, sleep disturbance, and restlessness likewise cross diagnostic boundaries.
Clinical research indicates that ADHD is frequently diagnosed later in individuals who first present with anxiety or depression, particularly in adults and especially in women. The ADHD may have been present since childhood but was attributed to "nervousness," "sensitivity," or "not applying oneself." Meanwhile, the person developed elaborate coping mechanisms that partially compensated for executive function deficits—until life demands exceeded their compensatory capacity, triggering anxiety and depression.
Conversely, some individuals receive an ADHD diagnosis without adequate recognition of co-occurring mood disorders. Treatment focused exclusively on ADHD symptoms may provide partial relief but fail to address the anxiety and depression that have become independent problems requiring their own intervention.
Distinguishing features that may help clarify the diagnostic picture:
- ADHD symptoms typically have childhood onset, even if not recognized at the time, while pure anxiety or depression often emerge later
- ADHD-related difficulties appear across multiple contexts, while situational anxiety may be more domain-specific
- Core ADHD symptoms persist during periods of low stress, while pure anxiety/depression symptoms may remit when stressors resolve
- Response to treatment can be informative—improvement with ADHD-specific interventions suggests ADHD was contributing, though this doesn't rule out comorbidity
Healthcare providers with expertise in adult ADHD increasingly recognize the importance of comprehensive assessment that evaluates all three conditions and their interactions. This typically involves detailed developmental history, current symptom assessment across multiple domains, and careful attention to the temporal relationships between symptoms.
Effectively addressing the co-occurrence of ADHD with recurring anxiety depression requires interventions that target all three conditions and specifically disrupt the reinforcing cycles between them. Single-focus approaches—treating only the ADHD or only the depression—typically provide incomplete relief and leave individuals vulnerable to continuation of the cycle.
Creating External Structure to Support Internal Regulation
Individuals with ADHD benefit substantially from external structure that compensates for executive function challenges. When anxiety and depression are also present, establishing this structure becomes both more important and more difficult. Depression saps the motivation needed to create routines, while anxiety can lead to either rigid overplanning or avoidant underplanning.
Practical approaches include working with a coach, therapist, or accountability partner to establish minimal viable routines—not perfect systems, but basic structures that can be maintained even during low periods. This might mean setting only three non-negotiable daily anchors (medication time, one meal, bedtime) rather than attempting comprehensive scheduling.
Digital tools and apps designed for ADHD management can provide external reminders and structure. Similarly, on-demand support tools like Lovon.app can offer accessible opportunities to process stress and emotional patterns as they arise, potentially interrupting the escalation from temporary difficulty into full anxiety spirals.
Addressing Sleep as a Central Intervention Point
Sleep disturbance appears in ADHD (difficulty settling due to racing thoughts), anxiety (difficulty falling or staying asleep due to worry), and depression (disrupted sleep architecture, early waking). Poor sleep, in turn, worsens executive function, emotional regulation, and mood stability—amplifying all three conditions.
Research suggests that prioritizing sleep as a primary intervention target can create positive cascading effects across all three conditions. This involves working with healthcare providers to address any sleep disorders, establishing consistent sleep-wake times, and potentially discussing whether medication adjustments might improve sleep quality.
For some people, this may involve consultation with providers about supplements or medications that support sleep, though specific recommendations should always come from qualified healthcare professionals familiar with your complete health picture. The goal is stabilizing the sleep-wake cycle as a foundation for improving daytime functioning.
Cognitive and Behavioral Strategies Adapted for ADHD
Traditional cognitive-behavioral therapy (CBT) for anxiety and depression requires consistent homework completion, detailed thought records, and sustained focus—all challenging for individuals with ADHD. Adapted approaches acknowledge these challenges while maintaining therapeutic effectiveness.
CBT adapted for ADHD typically involves shorter, more frequent sessions, greater use of visual aids and concrete examples, built-in accountability structures, and modified homework that accommodates executive function challenges. The therapeutic relationship itself may emphasize more frequent check-ins and external support for implementing strategies.
Specific techniques that may help interrupt the anxiety-depression cycle include:
- Behavioral activation in small increments: Rather than attempting full activity scheduling, identifying one or two specific activities that provide accomplishment or pleasure and building from there
- Worry containment strategies: Designating specific "worry times" rather than attempting to eliminate anxious thoughts entirely—this acknowledges the difficulty with thought suppression while preventing worry from consuming the entire day
- Self-compassion practices: Explicitly addressing the harsh self-criticism that often develops from years of underperformance and may fuel both anxiety and depression
Talking through patterns, preparing for difficult situations, and gaining perspective on recurring cycles can be valuable—whether with a traditional therapist or through accessible tools like Lovon.app that allow processing in the moment when patterns emerge.
Considering Medication as Part of Comprehensive Treatment
While this article doesn't recommend specific medications or dosages, it's important to acknowledge that pharmacological treatment is often a valuable component of managing ADHD comorbidity with anxiety and depression cycles. The decision about whether and which medications to try should involve detailed consultation with healthcare providers who understand the full clinical picture.
Some individuals benefit from treating the ADHD directly, finding that improved executive function and attention reduce the circumstances that generate anxiety and depression. Others require treatment targeting anxiety or depression as primary concerns, with ADHD addressed secondarily or simultaneously. Still others need integrated approaches that address all three conditions.
The complexity lies in the fact that some medications used for one condition may affect others—sometimes helpfully, sometimes problematically. Stimulant medications for ADHD, for instance, can sometimes worsen anxiety in certain individuals, while for others they reduce anxiety by improving functioning. Antidepressants may help both depression and anxiety but might not address core ADHD symptoms. Working with prescribers who understand these interactions and can monitor responses carefully is essential.
Given the complexity of managing co-occurring ADHD, anxiety, and depression—especially when they create reinforcing cycles—professional support is typically necessary. The question is often not whether to seek help but what kind and from whom.
Comprehensive assessment by providers familiar with adult ADHD and its common comorbidities provides the foundation for effective treatment. This might involve psychiatrists, clinical psychologists, or other mental health professionals with specific training in ADHD and mood disorders. The assessment process should include detailed developmental history, current symptom presentation across multiple life domains, and evaluation for other potential contributing factors.
Red flags that indicate immediate professional help is needed include thoughts of self-harm, inability to meet basic self-care needs, substance use to cope with symptoms, or significant impairment in major life areas (work, relationships, self-care). These situations require prompt clinical intervention, not self-management alone.
For ongoing management, effective treatment teams often include multiple providers: a prescriber who manages medications, a therapist who provides CBT or other evidence-based counseling, and potentially a coach who helps with practical skill-building and accountability. Some people also find peer support groups specifically for adults with ADHD valuable for reducing isolation and sharing practical strategies.
Between formal appointments, having accessible resources for processing emotions and working through challenges can help maintain progress. This is where on-demand tools that allow talking through patterns and preparing for difficult situations can complement traditional treatment, providing support during the substantial time between scheduled sessions.
Beyond formal treatment, individuals managing the co-occurrence of ADHD with recurring anxiety depression benefit from practical daily strategies that accommodate all three conditions:
Morning routines that support all three conditions:
- Keep morning complexity minimal—too many steps increase ADHD-related failure and anxious overwhelm
- Include brief physical movement, which research suggests may help mood, attention, and anxiety
- Build in transition time between waking and demands, allowing the executive function system to come online gradually
Throughout the day:
- Use external cues and reminders rather than relying on memory and internal time sense
- Break tasks into smaller components that provide more frequent accomplishment moments—countering depressive discouragement while making tasks less overwhelming for ADHD-challenged planning
- Schedule brief breaks before reaching depletion—preventing the crash that triggers depressive withdrawal
Recognizing early cycle signals:
- Identify personal early warning signs that the anxiety-depression cycle is beginning (for some this is sleep changes, for others it's irritability or withdrawal)
- Have a predetermined "early intervention plan" ready to implement when these signals appear—making decisions in advance, when executive function is less impaired
- Share these signals with trusted others who can provide external observation and support
Evening routines:
- Establish consistent wind-down that signals transition toward sleep (supporting both ADHD-related circadian tendencies and anxiety-related hyperarousal)
- Offload worries and planning thoughts externally (paper, app, voice memo) rather than attempting to hold them mentally
- Practice brief gratitude or positive reflection—even small moments—to counter depressive negative bias without demanding lengthy exercises that ADHD makes difficult to sustain
The goal isn't perfect implementation but rather having accessible strategies that match the real capacities and challenges of managing three interacting conditions.
ADHD comorbidity with anxiety and depression cycles represents one of the most common and challenging presentations in adult mental health. The cycle emerges naturally from the interaction between ADHD-related functional impairments, the anxiety these difficulties generate, and the depression that develops from chronic stress and repeated experiences of underperformance. Each condition worsens the others, creating reinforcing patterns that can feel inescapable.
Yet understanding these patterns is itself the beginning of change. Recognizing that the cycle is predictable—that it follows certain patterns and involves specific mechanisms—makes it possible to intervene at multiple points. Effective management requires comprehensive assessment, treatment that addresses all three conditions rather than focusing on only one, and daily practical strategies adapted to accommodate executive function challenges while supporting mood stability.
This is not work that individuals must do alone. Professional support, appropriate treatment, practical tools, and accessible resources for processing patterns as they emerge all play valuable roles. Whether through traditional therapy, medication management, coaching, peer support, or accessible tools like Lovon.app for working through challenges between formal appointments, building a comprehensive support network matched to your specific presentation creates the best foundation for breaking cycles and building sustainable functioning.
If you're recognizing these patterns in your own experience, consider seeking comprehensive evaluation from providers familiar with ADHD and its common comorbidities. The cycle is common, understandable, and—with appropriate support and strategies—manageable.
This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm—seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
More articles by The Lovon Editorial Team
Similar Articles
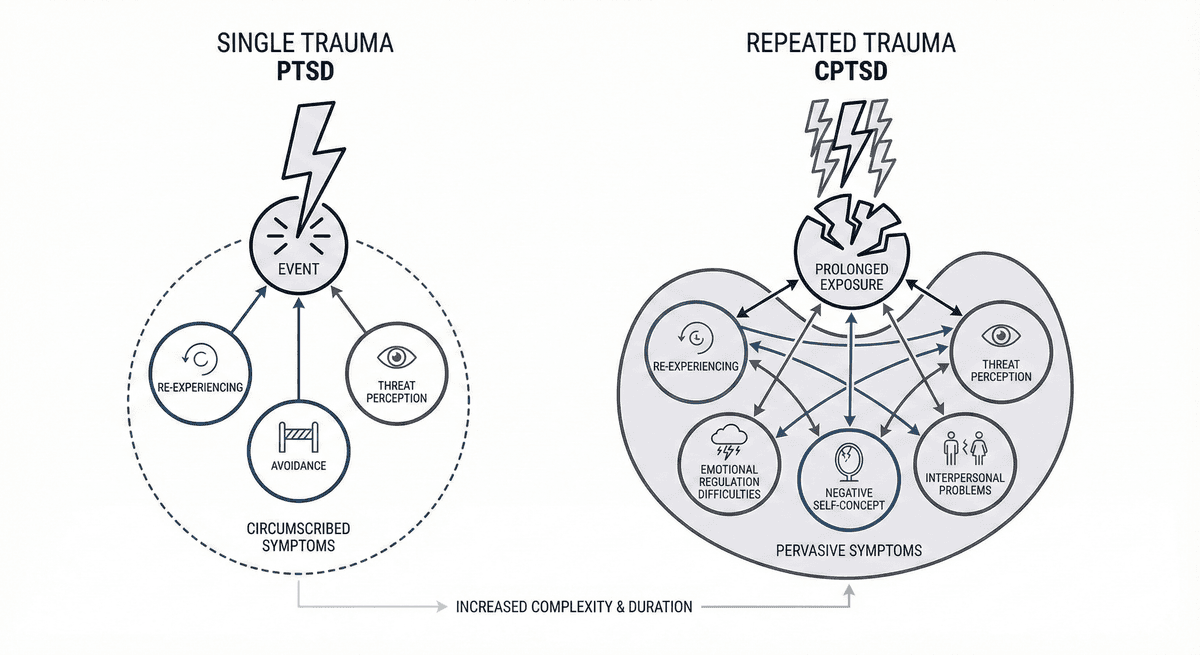
PTSD vs CPTSD: Single Trauma vs Repeated Trauma Symptom Differences
Learn how PTSD from a single traumatic event differs from CPTSD shaped by repeated trauma, including symptom patterns and treatment approaches.
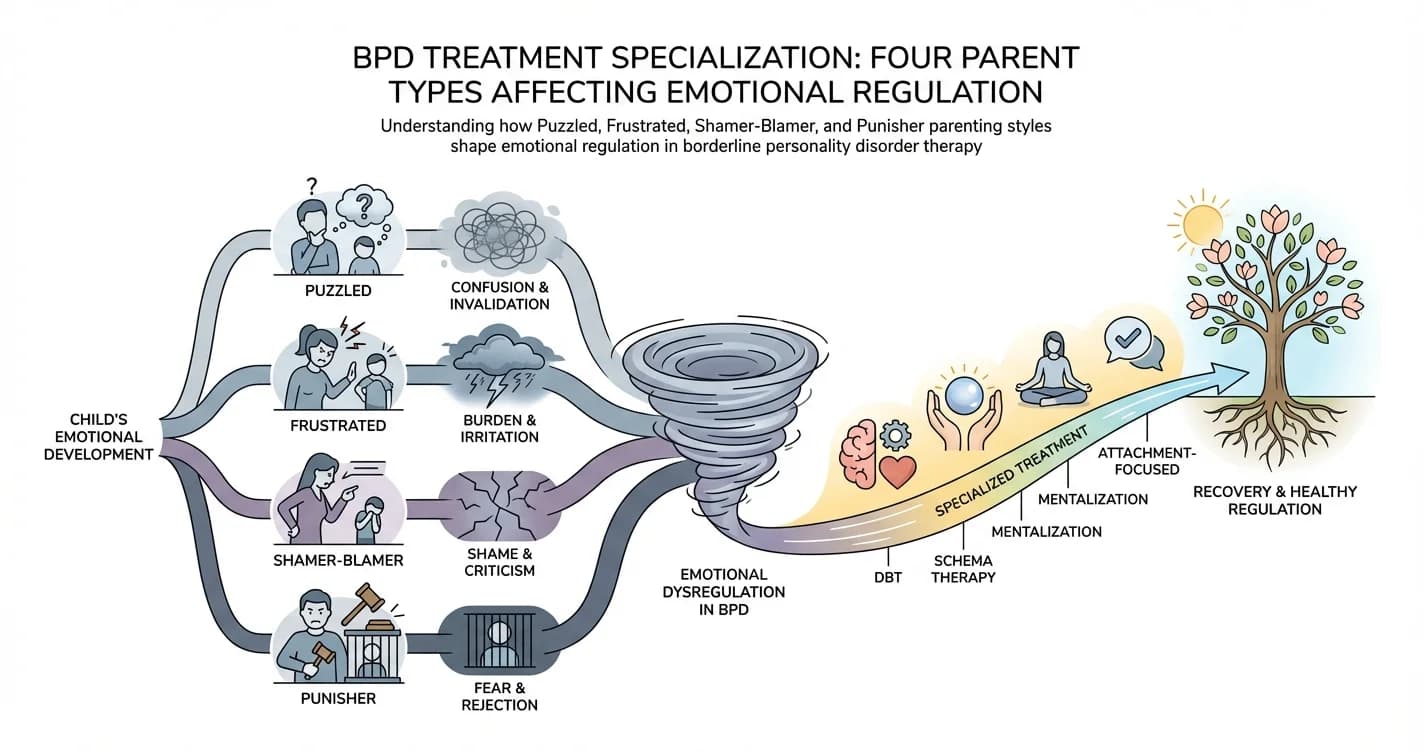
BPD Treatment Specialization: Four Parent Types Affecting Emotional Regulation
For individuals with borderline personality disorder (BPD), emotional regulation difficulties rarely emerge in isolation. Research increasingly suggests that
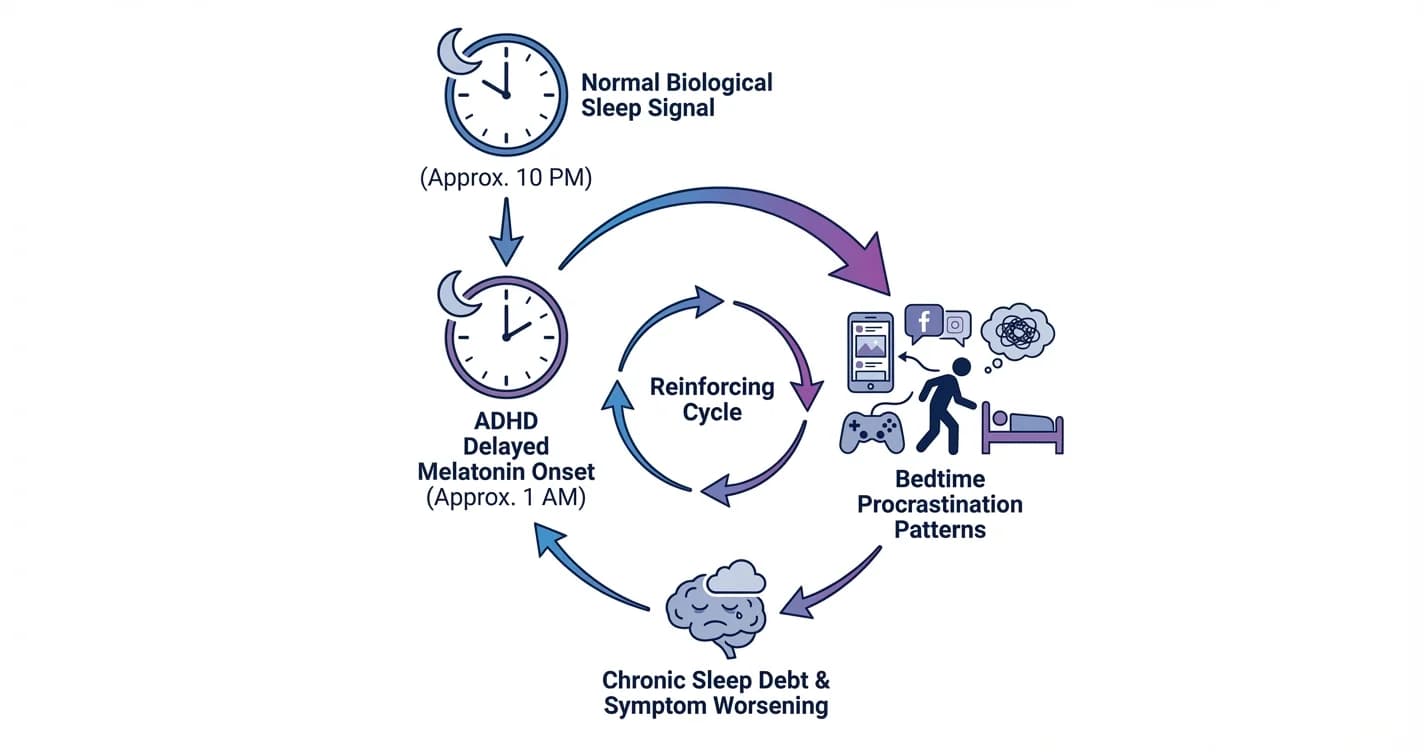
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.