Understanding the Four PTSD Symptom Categories: Reexperiencing, Trigger Reactivity, Mood Alterations, and Altered Reactivity
A comprehensive guide to recognizing and understanding the core symptom groups that define post-traumatic stress disorder
Key Takeaways
- They help distinguish normal stress responses from clinical PTSD requiring professional intervention
- Each category may respond differently to various therapeutic approaches
- Recognizing patterns across categories can validate confusing experiences
- They provide a framework for tracking symptom changes over time
- Places associated with the trauma or that share features with the traumatic location
Introduction
Post-traumatic stress disorder (PTSD) affects millions of people who have experienced or witnessed traumatic events, yet its symptoms often manifest in ways that aren't immediately recognized as trauma-related. Understanding the four PTSD symptom categories—reexperiencing, trigger reactivity, mood alterations, and altered reactivity—provides essential insight into how trauma reshapes cognitive and emotional functioning. These distinct yet interconnected symptom groups form the diagnostic framework mental health professionals use to identify PTSD, and recognizing them can be the first step toward appropriate support. This article explores each category in depth, drawing on current clinical understanding to help you recognize these patterns whether you're experiencing them yourself or supporting someone who is.
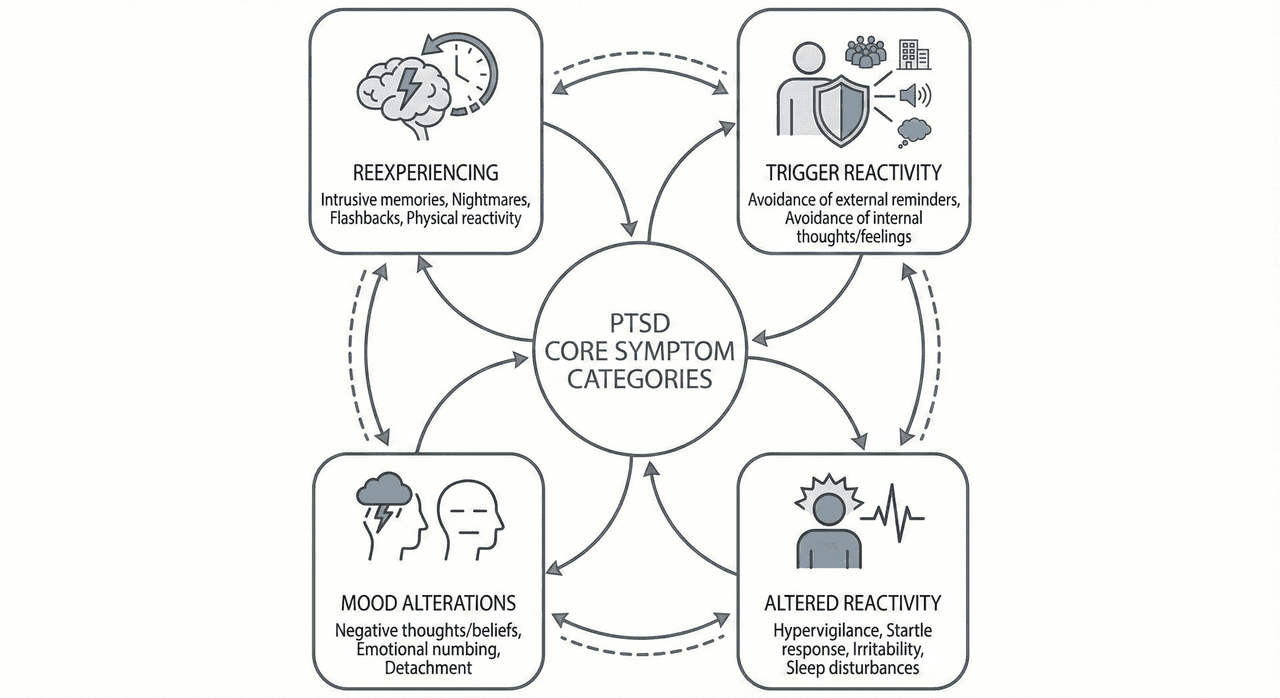
The Clinical Framework of PTSD Symptom Categories
Mental health professionals organize PTSD symptoms into four distinct categories that reflect different ways trauma affects psychological functioning. This classification system, outlined in diagnostic criteria used by clinicians, helps differentiate PTSD from other stress-related conditions and guides treatment approaches.
The four PTSD symptom categories—reexperiencing, trigger reactivity, mood alterations, and altered reactivity—each represent different aspects of how the nervous system and mind respond to overwhelming traumatic experiences. Research from institutions like the National Institute of Mental Health indicates that these categories aren't mutually exclusive; most people with PTSD experience symptoms across multiple categories, though the severity and specific manifestations vary considerably between individuals.
Understanding these categories matters because:
- They help distinguish normal stress responses from clinical PTSD requiring professional intervention
- Each category may respond differently to various therapeutic approaches
- Recognizing patterns across categories can validate confusing experiences
- They provide a framework for tracking symptom changes over time
The presence of symptoms from all four categories, persisting for more than a month and causing significant distress or functional impairment, typically indicates PTSD rather than a normal adjustment response to stress.
Reexperiencing: When the Past Invades the Present
Reexperiencing symptoms represent the mind's involuntary replay of traumatic memories, often with the same emotional and physical intensity as the original event. This category distinguishes PTSD from other anxiety conditions—the trauma doesn't stay in the past but intrudes repeatedly into present consciousness.
Common Forms of Reexperiencing
Intrusive memories emerge without warning, often triggered by sensory cues that share features with the traumatic event. Unlike normal memories that feel like recollections, intrusive memories can feel like the event is happening again, complete with sensory details—sights, sounds, smells, physical sensations—that accompanied the trauma.
Nightmares and trauma-related dreams disrupt sleep and may involve direct replays of the event or thematically related scenarios. Some people experience recurring nightmares with identical content, while others have variations that share emotional themes with the trauma. The distress often continues after waking, affecting the willingness to return to sleep.
Flashbacks represent the most intense form of reexperiencing, where the person temporarily loses awareness of current surroundings and feels transported back to the traumatic moment. During flashbacks, present-moment sensory information is overridden by traumatic memories. These episodes vary in duration from seconds to minutes and can involve complete disorientation about time and place.
Physical reactivity to reminders manifests as sudden increases in heart rate, sweating, rapid breathing, or muscle tension when encountering trauma-related cues. The body responds as though facing immediate danger even when the conscious mind recognizes safety.
Why Reexperiencing Occurs
The brain appears to process traumatic memories differently than ordinary experiences. During overwhelming events, normal memory consolidation processes may be disrupted, leaving traumatic information "unprocessed" in a way that makes it accessible to involuntary recall with full emotional intensity. This neurological response developed as a survival mechanism—remembering danger in vivid detail helps avoid similar threats—but becomes problematic when the system remains hyperactivated long after danger has passed.
Trigger Reactivity: Avoidance and the Narrowing of Life
The second symptom category involves persistent avoidance of trauma-related stimuli and intense efforts to prevent reexperiencing symptoms. This category reflects how people with PTSD actively attempt to manage their symptoms by limiting exposure to reminders, often at significant cost to daily functioning.
External Avoidance Patterns
People may avoid:
- Places associated with the trauma or that share features with the traumatic location
- People who were present during the event or who might discuss it
- Activities that might trigger memories, even if previously enjoyed
- Sensory experiences like certain sounds, smells, or visual stimuli
- Media content depicting similar events or themes
These avoidance behaviors often expand over time as more situations become associated with the trauma through generalization. Someone who experienced a car accident might initially avoid the accident location, then all highways, then eventually all driving.
Internal Avoidance Strategies
Beyond avoiding external reminders, trigger reactivity includes efforts to avoid internal experiences:
- Thought suppression: Actively trying not to think about the trauma, which paradoxically often increases intrusive thoughts
- Emotional numbing: Attempting to "shut down" feelings entirely to avoid trauma-related emotions
- Memory avoidance: Resisting any attempt to recall details of the event, even in therapeutic contexts
- Substance use: Using alcohol, drugs, or excessive work/activity to avoid processing trauma
While avoidance provides short-term relief from distressing symptoms, it prevents the natural processing that helps integrate traumatic experiences. Clinical approaches often gently challenge avoidance patterns, helping people gradually approach trauma-related material in controlled, safe contexts.
The Impact on Daily Life
Avoidance behaviors significantly narrow life experiences. People may withdraw from relationships, abandon careers, stop engaging in hobbies, or develop increasingly restricted routines designed to minimize potential triggers. This constriction itself becomes distressing, creating a secondary layer of loss beyond the original trauma. Tools like Lovon.app can provide accessible support for processing avoidance patterns between therapy sessions, offering a space to explore when and why certain situations feel overwhelming.
Mood Alterations: The Emotional Landscape After Trauma
The third category encompasses negative changes in thoughts and mood associated with the traumatic event. These cognitive and emotional alterations often develop or worsen after the trauma and represent how PTSD affects one's internal experience and worldview.
Cognitive Changes
Distorted beliefs about oneself, others, and the world emerge as the mind attempts to make sense of traumatic experiences. Common patterns include:
- Pervasive self-blame: "It was my fault" or "I should have prevented it"
- Generalized danger beliefs: "The world is completely unsafe" or "No one can be trusted"
- Diminished future expectations: "Nothing good will ever happen again"
- Negative self-concept: "I'm permanently damaged" or "I'm weak for being affected this way"
These beliefs feel absolutely true to the person experiencing them, even when others recognize them as distortions. They arise from the brain's attempt to create a coherent narrative from an overwhelming experience and to establish a sense of control—"If it was my fault, then I have power to prevent future harm."
Emotional Numbing and Detachment
Many people with PTSD experience a persistent inability to experience positive emotions—a phenomenon sometimes described as emotional numbing. Joy, love, satisfaction, and contentment feel distant or completely inaccessible. This isn't simply sadness; it's more like emotional flatness or disconnection.
Detachment from others manifests as feeling fundamentally separate from other people, even loved ones. Social interactions may feel like going through motions without genuine connection. This detachment serves a protective function—limiting emotional investment reduces vulnerability—but isolates people from support systems when they need them most.
Persistent Negative Emotional States
Beyond numbing, mood alterations include sustained experiences of:
- Fear and horror that persist beyond the trauma context
- Anger and irritability that feel disproportionate to situations
- Shame and guilt connected to the trauma or its aftermath
- Sadness and grief for what was lost—safety, trust, previous sense of self
These aren't temporary mood fluctuations but persistent emotional states that color all experiences. The person may struggle to remember feeling any other way, even though these states intensified after the trauma.
Memory Difficulties
Some people with PTSD experience inability to recall important aspects of the traumatic event. This isn't ordinary forgetting but rather dissociative amnesia—the brain protects itself by blocking access to certain memories. Paradoxically, the person may be flooded with intrusive memories of some trauma aspects while unable to recall other details, creating a fragmented, confusing narrative.
Altered Reactivity: Changes in Arousal and Physical Response
The fourth category—altered arousal and reactivity—describes how PTSD affects the nervous system's baseline state and responsiveness. People with these symptoms exist in a persistent state of physiological hyperactivation, as though the body hasn't received the message that danger has passed.
Hypervigilance and Exaggerated Startle Response
Hypervigilance involves constantly scanning the environment for potential threats, maintaining exhausting levels of attention to surroundings. In social settings, this might look like choosing seats with clear views of exits, repeatedly checking doors and windows, or difficulty concentrating on conversations while monitoring the environment.
Exaggerated startle response means reacting with disproportionate intensity to unexpected stimuli—jumping dramatically at sudden noises, loud voices, or unexpected touch. The body responds to minor stimuli as though they signal immediate danger, flooding the system with stress hormones before conscious awareness can assess the actual threat level.
Sleep Disturbances
PTSD profoundly affects sleep through multiple mechanisms:
- Difficulty falling asleep due to hyperarousal—the body and mind can't settle enough to permit sleep onset
- Frequent awakening throughout the night, often without clear cause
- Trauma-related nightmares that wake the person in acute distress
- Resistance to sleep itself, as sleep represents vulnerability and loss of control
These sleep problems compound other symptoms—sleep deprivation worsens emotional regulation, concentration, and physical health, creating a cycle where symptoms reinforce each other.
Irritability and Aggressive Behavior
Altered reactivity often includes irritability, angry outbursts, or aggressive behavior with minimal provocation. This doesn't reflect the person's character but rather a nervous system stuck in a defensive state. Small frustrations trigger disproportionate reactions because the system is already primed for threat response.
Family members and friends often find this symptom particularly challenging, as the person may seem unpredictably reactive or "on edge." The person experiencing these responses may feel equally distressed by their own reactions, experiencing shame or confusion about behaviors that feel out of character.
Reckless or Self-Destructive Behavior
Some people develop reckless or self-destructive patterns after trauma, including substance misuse, dangerous driving, promiscuous sexual behavior, or other high-risk activities. These behaviors may serve multiple functions: seeking stimulation intense enough to penetrate emotional numbing, self-medicating distress, or unconsciously testing survival or expressing diminished regard for personal safety.
Concentration Difficulties
Problems with concentration and memory stem from the cognitive resources consumed by hypervigilance and intrusive thoughts. When mental energy is devoted to threat monitoring and trauma processing, less remains available for everyday tasks. People may struggle to follow conversations, complete work tasks, or remember routine information—difficulties that can be misinterpreted as lack of interest or capability rather than trauma symptoms.
How the Four Categories Interact in Daily Life
Understanding the four PTSD symptom categories—reexperiencing, trigger reactivity, mood alterations, and altered reactivity—becomes most meaningful when considering how they interact and reinforce each other in daily experience.
A typical cycle might unfold like this: A sensory cue triggers reexperiencing (intrusive memory or physiological response), which activates altered reactivity (heart racing, hypervigilance increases). To prevent further reexperiencing, the person engages trigger reactivity (avoidance of similar situations), which confirms danger beliefs and maintains mood alterations (persistent fear, inability to experience safety). The chronic stress of this cycle worsens altered reactivity (sleep problems, irritability), which lowers the threshold for future reexperiencing symptoms.
Professional treatment approaches, including trauma-focused therapies, work by interrupting these reinforcing cycles at multiple points. Between formal therapy sessions, accessible support tools like Lovon.app can help process day-to-day experiences and maintain awareness of symptom patterns, offering a space to reflect on what's triggering and why.
Individual Variation in Symptom Presentation
While diagnostic criteria require symptoms from all four categories, the specific manifestations vary considerably. Some people experience predominantly internal symptoms (intrusive thoughts, emotional numbing), while others have more obvious behavioral changes (avoidance, irritability). Symptom intensity fluctuates in response to current stressors, anniversaries of trauma, or seemingly random factors.
This variation means two people with PTSD may have quite different day-to-day experiences. Neither presentation is more "valid" than the other—PTSD encompasses a wide range of trauma responses, all reflecting genuine suffering and impairment.
When to Seek Professional Support
If you recognize symptoms across the four PTSD symptom categories—reexperiencing, trigger reactivity, mood alterations, and altered reactivity—persisting for more than a month and significantly affecting your functioning, professional evaluation is appropriate. Effective treatments exist, including trauma-focused cognitive behavioral therapy and EMDR (Eye Movement Desensitization and Reprocessing), which show substantial evidence for reducing PTSD symptoms.
Early intervention generally produces better outcomes, though people can benefit from treatment regardless of how much time has passed since the trauma. The journey isn't linear—healing involves gradual processing of traumatic experiences and learning to regulate responses, rather than eliminating all distress.
Several factors indicate particularly urgent need for professional help:
- Thoughts of self-harm or suicide
- Substance use that's escalating or causing problems
- Inability to fulfill basic responsibilities at work or home
- Complete social withdrawal lasting weeks
- Dissociative episodes where you lose time or feel detached from reality
Remember that seeking help reflects strength and self-awareness, not weakness. Trauma responses are normal reactions to abnormal events—your symptoms represent your nervous system's attempt to protect you, even when those protective mechanisms have become problematic themselves.
Conclusion
The four PTSD symptom categories—reexperiencing, trigger reactivity, mood alterations, and altered reactivity—provide a comprehensive framework for understanding how trauma affects psychological and physiological functioning. Recognizing symptoms across these categories validates confusing experiences and points toward appropriate support. Reexperiencing brings the past involuntarily into the present; trigger reactivity involves avoiding reminders at increasing cost; mood alterations reflect changed beliefs and emotional capacity; altered reactivity represents a nervous system stuck in threat response mode.
These categories aren't separate problems but interconnected aspects of trauma response that reinforce each other. Understanding this complexity helps explain why PTSD feels so consuming and why effective treatment addresses multiple symptom types simultaneously. Whether you're experiencing these symptoms yourself or supporting someone who is, recognizing the patterns is the first step toward appropriate help. Professional treatment offers the most comprehensive support, while tools like accessible therapy options and on-demand resources provide additional layers of care during the recovery process.
This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm—seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
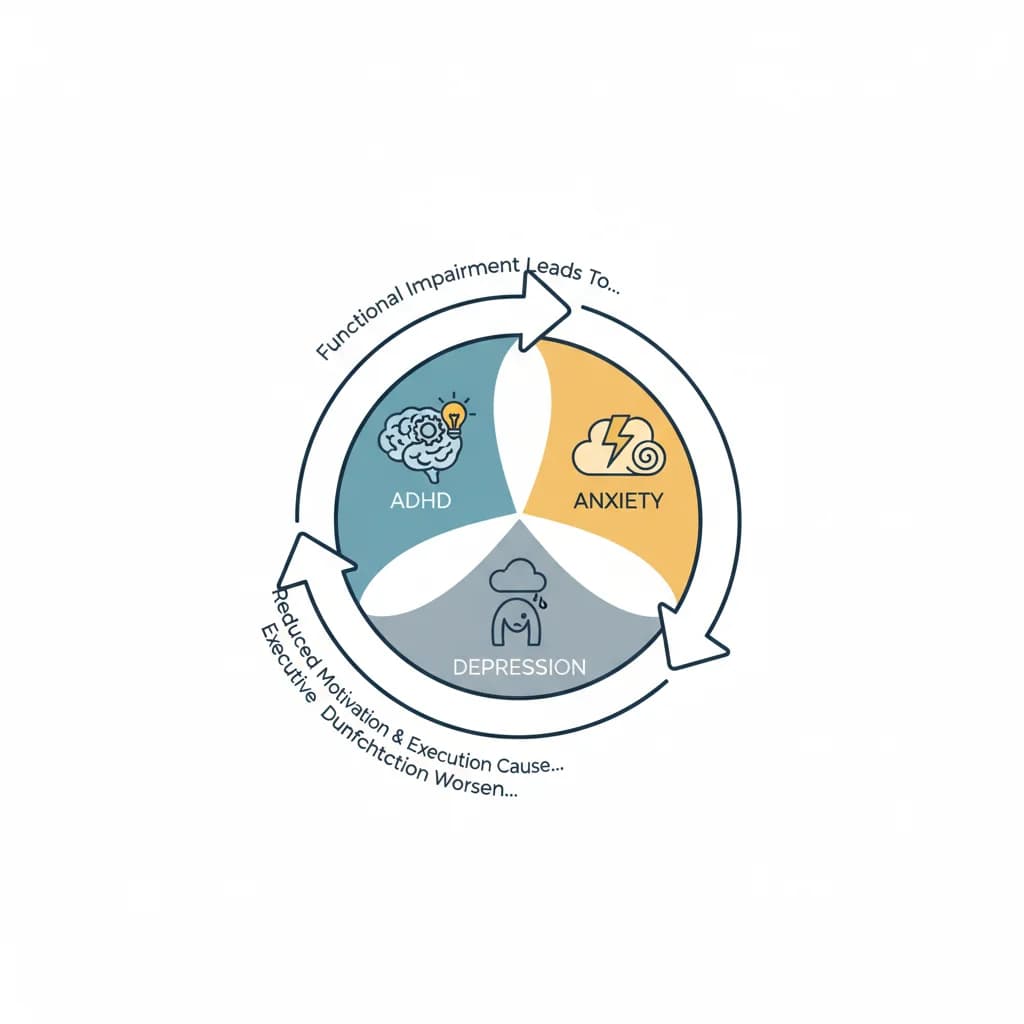
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
BPD Treatment Specialization: Four Parent Types Affecting Emotional Regulation
For individuals with borderline personality disorder (BPD), emotional regulation difficulties rarely emerge in isolation. Research increasingly suggests that
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.