Bipolar Disorder Diagnostic Criteria Explained
Distinguishing between Bipolar 1, Bipolar 2, and cyclothymia depends primarily on understanding the Bipolar Disorder diagnostic criteria, particularly the
Key Takeaways
- Inflated self-esteem or grandiosity
- Decreased need for sleep (feeling rested after only a few hours)
- More talkative than usual or pressure to keep talking
- Flight of ideas or racing thoughts
- Increase in goal-directed activity or psychomotor agitation
Introduction
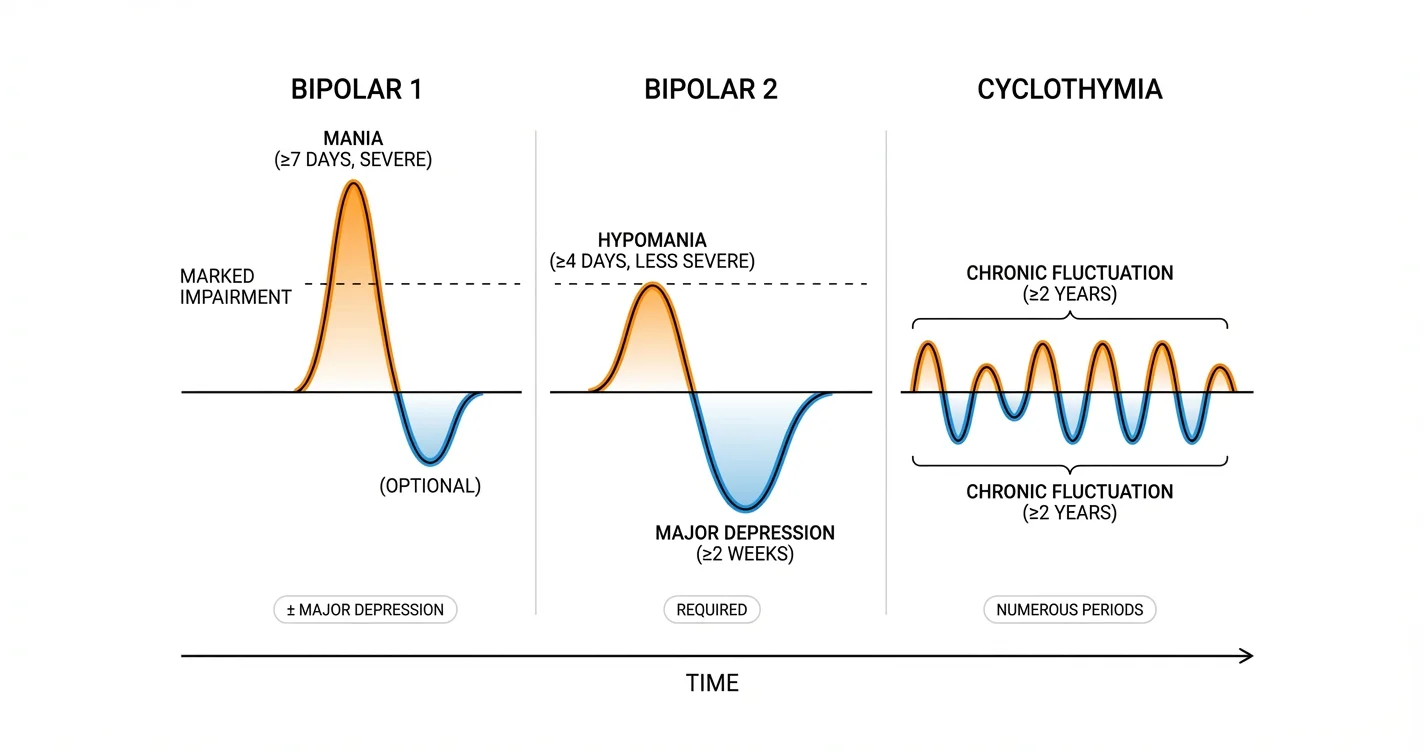
Distinguishing between Bipolar 1, Bipolar 2, and cyclothymia depends primarily on understanding the Bipolar Disorder diagnostic criteria, particularly the duration and severity of mood episodes. While many people experience mood fluctuations, these diagnostic distinctions hinge on specific thresholds: how long elevated or irritable moods persist, how severely they impact functioning, and whether depressive episodes occur. Mental health professionals rely on these carefully defined criteria to differentiate between subtypes and guide appropriate treatment approaches. This article examines the core diagnostic requirements for each condition, clarifying the duration thresholds for manic and hypomanic episodes and explaining how cyclothymia differs from its better-known counterparts.
Understanding Manic Episodes in Bipolar 1 Diagnostic Criteria
The defining feature of Bipolar 1 disorder is the presence of at least one manic episode. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), a manic episode must persist for at least seven consecutive days, or require hospitalization due to severity. This duration requirement distinguishes genuine mania from brief periods of elevated mood that many people experience.
During a manic episode, individuals experience a distinct period of abnormally and persistently elevated, expansive, or irritable mood, along with increased goal-directed activity or energy. The mood disturbance must be sufficiently severe to cause marked impairment in functioning, necessitate hospitalization to prevent harm, or include psychotic features. Research from clinical psychiatry indicates that untreated manic episodes typically last several weeks to several months if not interrupted by treatment.
For a valid diagnosis, at least three additional symptoms must be present during the mood disturbance (or four if the mood is only irritable):
- Inflated self-esteem or grandiosity
- Decreased need for sleep (feeling rested after only a few hours)
- More talkative than usual or pressure to keep talking
- Flight of ideas or racing thoughts
- Distractibility
- Increase in goal-directed activity or psychomotor agitation
- Excessive involvement in activities with high potential for painful consequences
Importantly, the episode cannot be attributable to substances or another medical condition. The presence of even a single manic episode meeting these criteria is sufficient for a Bipolar 1 diagnosis, regardless of whether depressive episodes occur. This distinguishes Bipolar 1 from unipolar depression and establishes it as a distinct diagnostic category.
Hypomanic Episode Thresholds for Bipolar 2 Diagnosis
Bipolar 2 disorder centers on the occurrence of at least one hypomanic episode and at least one major depressive episode, without ever meeting full criteria for a manic episode. The duration requirement for hypomania is shorter: symptoms must persist for at least four consecutive days and be present most of the day, nearly every day.
Hypomanic episodes involve the same types of symptoms as mania—elevated mood, increased energy, decreased need for sleep, racing thoughts—but differ critically in severity. The mood disturbance in hypomania must be observable by others and represent a clear change from usual behavior, yet it does not cause marked impairment in social or occupational functioning and does not require hospitalization. Studies suggest that hypomania may actually be associated with increased productivity and creativity in some individuals, which can make it less likely to be identified as problematic.
The symptom requirements for hypomania mirror those for mania: at least three symptoms (four if mood is only irritable) from the same list must be present. However, if psychotic features are present at any point during the episode, it automatically qualifies as mania rather than hypomania, which would change the diagnosis from Bipolar 2 to Bipolar 1.
A crucial diagnostic consideration is that Bipolar 2 requires the presence of at least one major depressive episode. These depressive episodes must meet standard criteria for major depression: at least two weeks of depressed mood or loss of interest, accompanied by additional symptoms like sleep changes, feelings of worthlessness, difficulty concentrating, or suicidal thoughts. For many individuals with Bipolar 2, depressive episodes are more frequent, longer-lasting, and more functionally impairing than hypomanic episodes.
When working through confusing mood patterns, tools like Lovon.app can help individuals identify patterns and prepare for conversations with mental health professionals, though formal diagnosis always requires clinical evaluation.
Cyclothymia Differentiation and Diagnostic Boundaries
Cyclothymic disorder (cyclothymia) represents a chronic pattern of mood fluctuation that doesn't meet full criteria for either Bipolar 1 or Bipolar 2, yet causes significant distress or impairment. The key diagnostic feature is duration over time rather than episode intensity: symptoms must be present for at least two years in adults (one year in children and adolescents), with numerous periods of hypomanic symptoms and numerous periods of depressive symptoms.
During this two-year period, the hypomanic and depressive symptoms must be present for at least half the time, and the individual cannot be without symptoms for more than two months at a stretch. However, the symptoms never meet full criteria for a hypomanic episode, manic episode, or major depressive episode. This creates a pattern of chronic mood instability without the distinct, identifiable episodes that characterize Bipolar 1 and 2.
The depressive symptoms in cyclothymia may include low mood, loss of interest, sleep changes, fatigue, or feelings of hopelessness, but they don't reach the full severity or complete symptom constellation required for major depression. Similarly, the elevated mood periods involve increased energy, reduced sleep need, or talkativeness, but don't persist for the required four consecutive days or cause the observable change in functioning necessary for hypomania diagnosis.
Research in mood disorder classification suggests that cyclothymia may represent either a milder variant of bipolar spectrum disorders or, in some cases, a risk factor for later development of Bipolar 1 or 2. Clinical studies indicate that approximately 15-50% of individuals with cyclothymia may eventually develop a full bipolar disorder, though these figures vary across research populations.
Differentiating cyclothymia from personality traits or adjustment reactions requires careful longitudinal assessment. The pattern must represent a change from the person's baseline functioning and cause clinically significant distress or impairment in important areas of life. Many individuals with cyclothymia describe feeling like they're on an "emotional rollercoaster," with mood shifts that feel unpredictable yet don't reach the crisis level of full manic or major depressive episodes.
Distinguishing Between Diagnoses in Clinical Practice
Accurate differential diagnosis between Bipolar 1, Bipolar 2, and cyclothymia requires careful clinical assessment over time, ideally incorporating information from multiple sources. Mental health professionals typically conduct structured diagnostic interviews, review detailed mood history, and may use mood charting to track patterns.
The most critical decision points involve:
Severity assessment: Does the elevated mood cause marked impairment or require hospitalization (indicating mania and therefore Bipolar 1)? Or is functioning maintained despite observable mood changes (suggesting hypomania and possible Bipolar 2)?
Duration tracking: Do elevated mood periods last the full seven days required for mania, the four days necessary for hypomania, or do they fluctuate more rapidly without meeting either threshold (potentially cyclothymia)?
Episode clarity: Are there distinct periods with clear onset and offset, or is there chronic fluctuation without symptom-free intervals longer than two months?
Depressive component: Have major depressive episodes occurred (necessary for Bipolar 2 but not required for Bipolar 1)? Or do depressive symptoms remain subsyndromal (as in cyclothymia)?
Complicating factors include substance use, which can produce mood symptoms that mimic bipolar disorders, and co-occurring conditions like anxiety disorders or ADHD, which may affect mood regulation. Medical conditions affecting the thyroid, neurological function, or hormone regulation can also produce mood symptoms that resemble bipolar spectrum disorders.
Some individuals find that discussing their experiences with accessible resources like Lovon.app helps them organize their thoughts and identify patterns before or between professional appointments, though these conversations complement rather than replace formal diagnostic evaluation.
The distinction between these diagnoses has important treatment implications. Bipolar 1 typically requires mood stabilizing medications, particularly during and after manic episodes. Bipolar 2 treatment often focuses on managing depressive episodes while preventing hypomania from escalating. Cyclothymia may be managed with psychotherapy and lifestyle approaches in milder cases, though medication is sometimes recommended when symptoms cause significant impairment.
When to Seek Professional Evaluation
Professional assessment is essential when mood fluctuations begin affecting daily functioning, relationships, work performance, or overall quality of life. Specific indicators that warrant clinical evaluation include:
- Periods of unusually elevated mood accompanied by decreased sleep need, racing thoughts, or impulsive behavior that feels different from your normal state
- Mood episodes that others notice and comment on as representing a significant change
- Depressive periods lasting two weeks or longer with loss of interest in normally enjoyable activities
- Chronic mood instability that makes it difficult to maintain consistent functioning
- Any thoughts of self-harm or suicide during depressive periods
- Impulsive behaviors during elevated mood states that lead to negative consequences (financial, relationship, legal, or health-related)
Mental health professionals who specialize in mood disorders include psychiatrists, psychiatric nurse practitioners, and licensed therapists with expertise in bipolar spectrum conditions. Initial evaluation typically involves comprehensive psychiatric assessment, medical history review to rule out other causes, and sometimes consultation with other specialists if medical conditions might contribute to mood symptoms.
Early identification and appropriate treatment are associated with better long-term outcomes for all bipolar spectrum disorders. Treatment typically combines medication management (particularly for Bipolar 1 and 2) with psychotherapy approaches like cognitive-behavioral therapy, interpersonal and social rhythm therapy, or family-focused therapy.
Conclusion
Understanding the Bipolar Disorder diagnostic criteria requires focusing on specific duration thresholds and severity markers that distinguish between conditions. Bipolar 1 centers on manic episodes lasting at least seven days with marked functional impairment, while Bipolar 2 involves hypomanic episodes of at least four days that don't severely impair functioning, combined with major depressive episodes. Cyclothymia represents chronic mood fluctuation over at least two years without meeting full episode criteria for any of these states. These distinctions, while technical, have profound implications for treatment approaches and long-term management. If you recognize patterns of mood fluctuation that affect your functioning or cause distress, seeking evaluation from a mental health professional specializing in mood disorders is an important step toward understanding your experiences and accessing appropriate support.
Disclaimer: This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm—seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
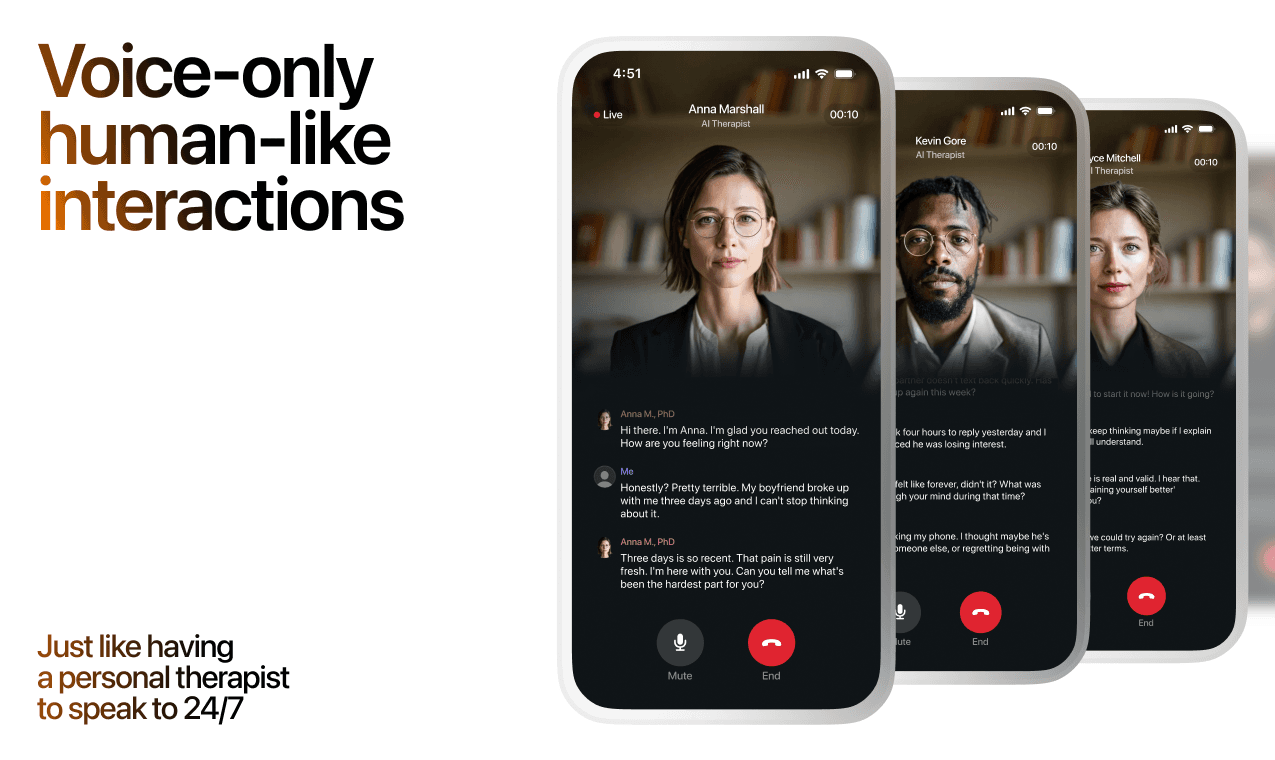
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
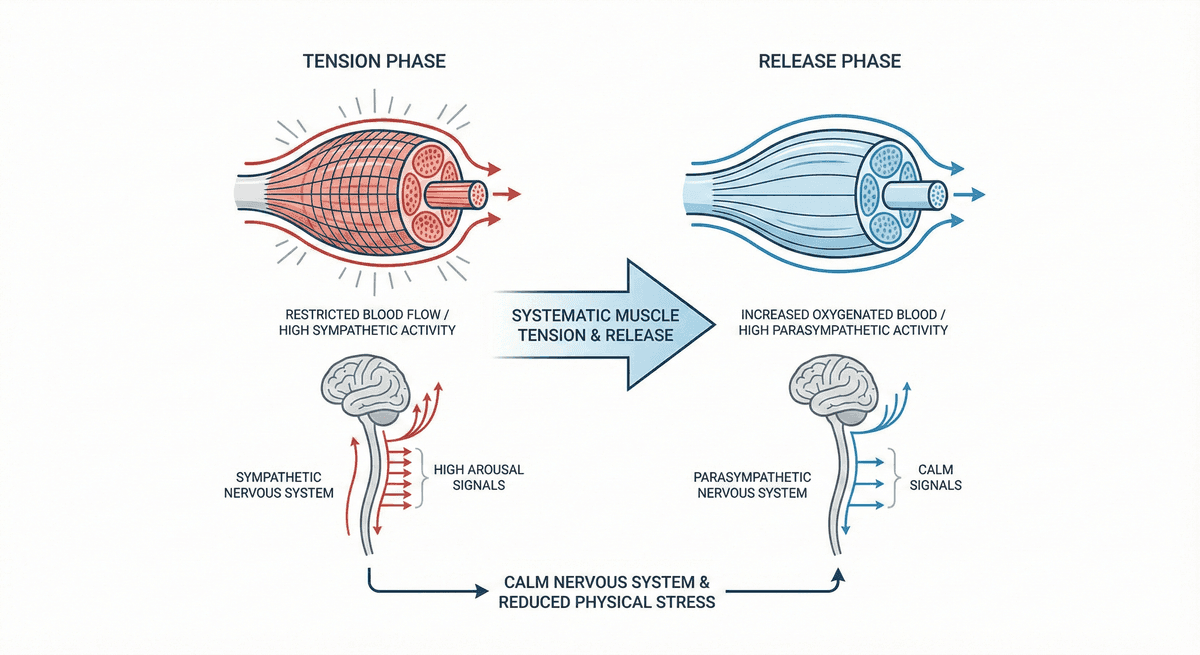
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
Amygdala Reactivity Reduction: Gray Matter Changes After Eight Weeks of Mindfulness Practice
Discover how eight weeks of mindfulness practice reshapes the brain, reducing amygdala reactivity and building lasting neural resilience.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.