PTSD vs CPTSD: Single Trauma vs Repeated Trauma Symptom Differences
Learn how PTSD from a single traumatic event differs from CPTSD shaped by repeated trauma, including symptom patterns and treatment approaches.
Key Takeaways
- PTSD often follows a single, time-limited event and symptoms tend to cluster around triggers tied to that incident.
- CPTSD typically arises from prolonged, repeated trauma and includes additional difficulties with emotion regulation, self-concept, and relationships.
- Treatment often differs: single-event PTSD may respond well to focused trauma processing, while CPTSD usually benefits from a phased, longer-term approach.
Understanding how one-time traumatic events and chronic trauma exposure shape distinct psychological responses and treatment needs.
Introduction
When someone experiences trauma, the psychological impact varies significantly depending on whether they faced a single, isolated incident or endured repeated traumatic experiences over time. The distinction between PTSD (Post-Traumatic Stress Disorder) and CPTSD (Complex Post-Traumatic Stress Disorder) centers on this fundamental difference—single trauma versus repeated trauma—and the symptom patterns that emerge from each. While both conditions involve distressing memories and heightened stress responses, CPTSD encompasses additional layers of emotional and relational difficulties that develop through prolonged exposure to inescapable situations. Understanding these differences is essential for recognizing symptoms, seeking appropriate support, and choosing treatment approaches that address the specific patterns each condition creates. This article examines the symptom variations between PTSD from one-time events and CPTSD from ongoing trauma, drawing on current clinical understanding and therapeutic approaches.
Understanding the Core Difference Between PTSD and CPTSD
The fundamental distinction between PTSD and CPTSD lies in the nature and duration of the traumatic exposure. PTSD typically develops following a discrete traumatic event—a car accident, natural disaster, assault, or combat incident—where the person experiences or witnesses something that threatens life or safety. The trauma has a clear beginning and end, even if the psychological impact continues long afterward.
CPTSD, by contrast, emerges from prolonged, repeated trauma, particularly in situations where escape feels impossible or where the trauma occurs during critical developmental periods. Research from institutions studying trauma psychology indicates that CPTSD commonly develops following experiences like childhood abuse, domestic violence, captivity, human trafficking, or long-term exposure to war zones. The repeated nature of the trauma, combined with the inability to escape, appears to fundamentally alter how individuals regulate emotions, relate to others, and perceive themselves.
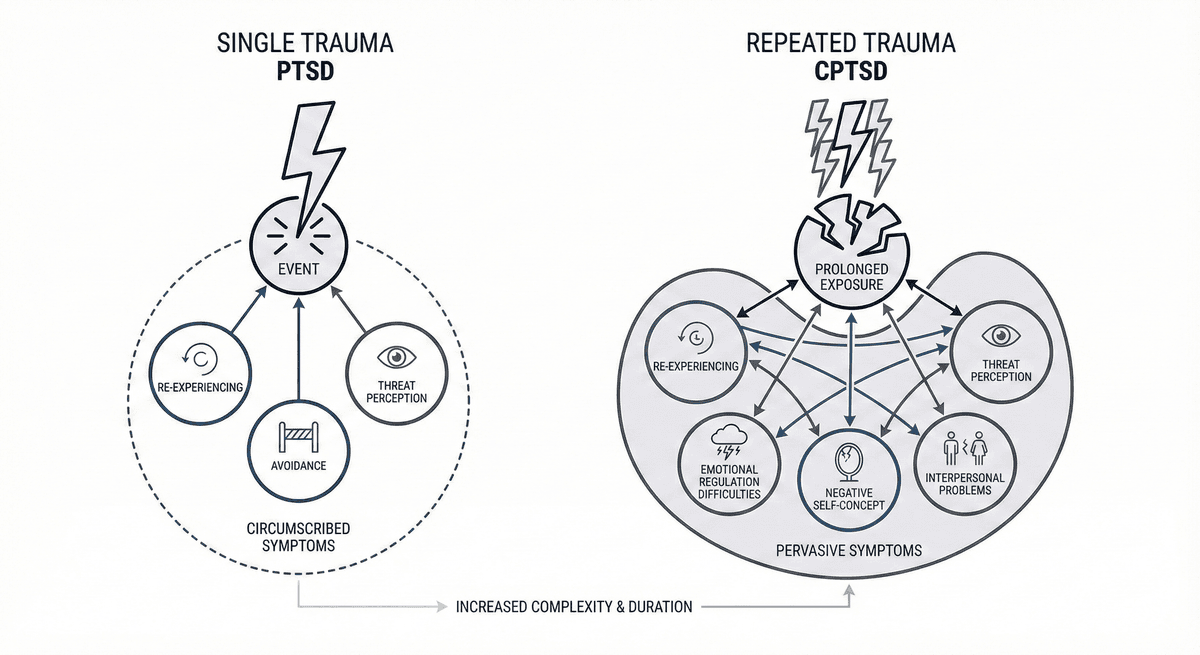
The World Health Organization's ICD-11 classification system formally recognized CPTSD as distinct from PTSD, acknowledging that the symptom profile extends beyond the core PTSD features. While PTSD centers on three main symptom clusters—re-experiencing the trauma, avoidance of reminders, and heightened threat perception—CPTSD includes these plus three additional categories related to disturbances in self-organization: emotional regulation difficulties, negative self-concept, and interpersonal problems.
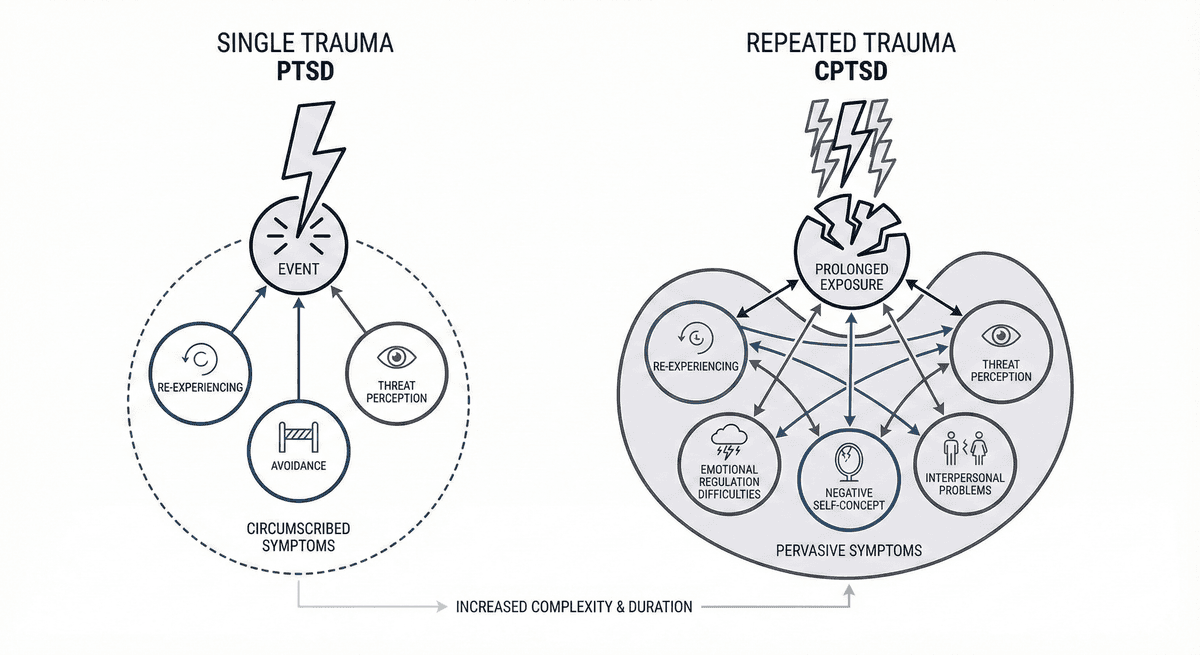
Comparison diagram showing differences between single trauma PTSD and repeated trauma CPTSD symptoms, illustrating how single-event PTSD has circumscribed symptoms connected to a specific incident, while repeated-trauma CPTSD involves pervasive, interconnected symptoms affecting emotion regulation, self-concept, and relationships
This distinction matters because it shapes treatment approaches. Someone with PTSD from a single trauma may respond well to trauma-focused therapies that process that specific event, while someone with CPTSD from repeated trauma typically requires longer-term treatment addressing relationship patterns, emotion regulation skills, and deeply held beliefs about self-worth developed through sustained traumatic experiences.
Single Trauma PTSD Symptoms: Patterns from One-Time Events
When PTSD develops following a single traumatic event, symptoms tend to cluster around that specific incident. The person's brain and nervous system remain on high alert for anything resembling the original threat, creating distinct patterns that interfere with daily functioning.
Core PTSD symptom categories include:
- Intrusive re-experiencing: Unwanted memories, nightmares, or flashbacks of the specific traumatic event appear suddenly and vividly, sometimes triggered by reminders but occasionally seeming to come from nowhere
- Avoidance behaviors: Deliberate efforts to avoid people, places, conversations, activities, or situations that might trigger memories of the trauma
- Negative thoughts and mood: Persistent negative beliefs about oneself, others, or the world that developed after the trauma, along with diminished interest in previously enjoyed activities
- Alterations in arousal and reactivity: Heightened startle response, difficulty sleeping, irritability, concentration problems, and hypervigilance—constantly scanning for potential threats
What distinguishes single-event PTSD is how these symptoms connect to a identifiable incident. A combat veteran might experience intense distress when hearing fireworks that sound like gunfire. Someone who survived a serious car accident may feel panic when approaching the intersection where it occurred. A person assaulted in a parking garage might avoid all parking structures and feel their heart race when walking through any enclosed space.
The timeline matters too. PTSD symptoms typically emerge within three months of the traumatic event, though sometimes they appear later. The intensity often peaks in the initial months, and for some people, symptoms gradually diminish over the first year even without formal treatment. However, for others—particularly without appropriate support—symptoms persist or worsen over time.
Importantly, people with single-trauma PTSD often maintain relatively intact abilities to regulate emotions outside of trauma-related situations. They may still form and maintain relationships, hold positive views of themselves in non-trauma domains, and function well in contexts that don't trigger reminders. The symptoms, while distressing and disruptive, tend to be more circumscribed around the specific traumatic experience rather than pervading all aspects of life.
Repeated Trauma CPTSD Symptoms: The Impact of Chronic Exposure
CPTSD from repeated trauma creates a more pervasive symptom pattern that extends beyond the core PTSD features. When someone experiences trauma repeatedly over months or years, particularly in situations where escape isn't possible, the psychological impact appears to fundamentally reshape emotional processing, self-perception, and relationship patterns.
In addition to the PTSD symptom clusters described above, CPTSD involves three additional categories of difficulties that research suggests emerge specifically from prolonged trauma exposure:
Emotion Regulation Difficulties
People with CPTSD often experience persistent problems managing emotional responses. This goes beyond the heightened reactivity seen in PTSD. Emotions may feel overwhelming, unpredictable, or difficult to understand. Some people describe feeling emotionally numb or disconnected, while others experience intense emotional swings that feel impossible to control. The capacity to self-soothe or return to emotional equilibrium after upset may be significantly impaired, likely because the skills for emotion regulation typically develop in safe, responsive environments—precisely what repeated trauma disrupts.
Negative Self-Concept
While PTSD may involve negative thoughts about oneself in relation to the trauma, CPTSD typically includes a more pervasive and deeply held sense of worthlessness, shame, or being fundamentally damaged. This isn't simply "I made a mistake" but rather "I am a mistake." People with CPTSD from childhood abuse, for instance, often internalize messages that they deserved the abuse or that something inherent about them is wrong. These beliefs become woven into identity rather than existing as thoughts about a specific event.
Interpersonal Difficulties
CPTSD commonly involves persistent challenges in relationships. Trust may feel impossible, particularly if the repeated trauma involved betrayal by someone in a caretaking or authority role. Some people withdraw from relationships entirely, feeling safer in isolation. Others may find themselves repeatedly entering harmful relationships, recreating familiar dynamics even when consciously desiring something different. The ability to feel safe with others, set appropriate boundaries, or maintain stable connections often requires specific therapeutic work to develop or rebuild.
The symptoms of CPTSD tend to be more constant and less tied to specific triggers than single-event PTSD. Rather than experiencing symptoms primarily when encountering reminders of a particular incident, people with CPTSD may experience ongoing emotional dysregulation, relationship difficulties, and negative self-perception across many situations. The trauma has become, in a sense, a lens through which all experiences are filtered.
Comparing PTSD and CPTSD Symptom Variations in Treatment Contexts
The symptom differences between PTSD from single trauma and CPTSD from repeated trauma have significant implications for treatment approaches and recovery trajectories. Recognizing these variations helps both individuals and clinicians understand what kind of therapeutic support might be most beneficial.
For single-event PTSD, trauma-focused therapies that process the specific traumatic memory often produce significant symptom reduction. Approaches that help the person revisit and reprocess the traumatic event in a safe therapeutic context can reduce the memory's emotional intensity and the associated avoidance and hyperarousal symptoms. Many people with PTSD from single traumas can engage effectively with these focused interventions and may experience substantial improvement in relatively shorter treatment timeframes—though "shorter" still typically means several months of consistent work.
CPTSD from repeated trauma generally requires a more comprehensive, phased approach. Studies examining trauma treatment approaches suggest that jumping immediately into trauma processing may be overwhelming or destabilizing for someone whose emotion regulation capacities were disrupted by prolonged trauma. Instead, treatment often begins with what clinicians call "stabilization"—developing skills for managing emotional responses, establishing safety in current life, and building the therapeutic relationship. Only once these foundations exist does trauma processing typically begin, and even then it may proceed more gradually.
The relationship component also differs significantly. For single-event PTSD, the therapeutic relationship matters, but the primary work centers on processing the trauma. For CPTSD, the therapeutic relationship itself becomes a crucial healing element—often the first experience of a safe, consistent, boundaried relationship where the person's needs and experiences are validated. This relational healing can't be rushed and contributes to why CPTSD treatment typically extends over longer periods.
Tools like Lovon.app can provide accessible support for processing emotions and recognizing patterns between formal therapy sessions, particularly for people working through relationship difficulties or preparing for challenging conversations. The on-demand nature allows people to talk through stressors as they arise, which can be especially valuable when building awareness of emotional patterns or relationship dynamics. However, particularly for CPTSD, these supportive resources work best as complements to, rather than replacements for, ongoing professional therapeutic relationships.
Recognizing Which Pattern You're Experiencing
Understanding whether your symptoms align more with single-trauma PTSD or repeated-trauma CPTSD can help guide decisions about seeking support and what approaches might be beneficial. Several factors can provide clues about which pattern may be present.
Consider the trauma history: If symptoms developed following a specific, identifiable incident—and there wasn't a history of previous or ongoing trauma—single-event PTSD is more likely. If the symptoms emerged during or after prolonged exposure to trauma, particularly during childhood or in situations involving captivity or ongoing relationship violence, CPTSD patterns are more probable.
Examine the symptom scope: Do symptoms primarily appear when encountering reminders of a specific event, or do emotional difficulties, relationship challenges, and negative self-perceptions pervade many areas of life regardless of specific triggers? The more pervasive and persistent the difficulties, particularly involving emotion regulation and relationship patterns, the more the presentation resembles CPTSD.
Assess relationship patterns: Can you generally form and maintain relationships outside of trauma-related contexts, or do relationship difficulties persist across different people and situations? Do you find yourself repeatedly encountering similar relationship problems despite consciously trying to create different outcomes? Pervasive interpersonal difficulties suggest the CPTSD pattern.
Reflect on self-concept: Are negative thoughts about yourself primarily connected to the trauma ("I should have acted differently during that event"), or do you experience a more fundamental sense of being damaged, worthless, or irreparably broken? The deeper, more identity-level negative self-concept points toward CPTSD.
It's important to note that these distinctions aren't always clear-cut. Some people experience multiple discrete traumas that together create a CPTSD-like presentation. Others may have primarily single-trauma PTSD but with some features more commonly associated with CPTSD. Clinical diagnosis considers the overall pattern and what treatment approach will likely be most helpful, rather than rigidly categorizing every presentation.
Professional assessment by a trauma-informed mental health provider can clarify which pattern best describes your experience and what treatment approaches are indicated. Many therapists now specifically train in both PTSD and CPTSD treatment protocols and can adjust their approach based on individual symptom profiles and trauma histories.
When to Seek Professional Support
Both PTSD from single trauma and CPTSD from repeated trauma warrant professional evaluation and treatment. While some people experience natural symptom reduction over time, particularly with social support and stable life circumstances, many find that symptoms persist or worsen without targeted intervention.
Consider seeking professional help if:
- Symptoms interfere with daily functioning, work, relationships, or activities you value
- You're using alcohol, substances, or other behaviors to manage distressing emotions or memories
- Avoidance patterns are narrowing your life—limiting where you go, who you see, or what you do
- Relationship difficulties are creating significant distress or instability
- You experience intense shame, worthlessness, or thoughts that others would be better off without you
- Sleep disturbances, concentration problems, or physical symptoms persist
For CPTSD specifically, finding a provider experienced in treating complex trauma is particularly valuable. Approaches like Dialectical Behavior Therapy (DBT) for emotion regulation skills, schema therapy for addressing deeply held negative beliefs, and various trauma-processing methods adapted for complex trauma can address the multiple layers of CPTSD symptoms.
Resources like Lovon.app can provide on-demand support for processing emotions and working through relationship concerns between therapy appointments, helping maintain momentum in therapeutic work. However, these tools complement rather than replace the structured, ongoing therapeutic relationship that CPTSD recovery typically requires.
Conclusion
The distinction between PTSD from single trauma versus CPTSD from repeated trauma reflects fundamentally different patterns of traumatic exposure and their psychological consequences. Single-event PTSD involves distressing re-experiencing, avoidance, and heightened threat perception centered around a specific incident, while CPTSD from repeated trauma encompasses these features plus pervasive difficulties with emotion regulation, negative self-concept, and interpersonal relationships. Recognizing these symptom differences matters because they point toward different treatment needs—focused trauma processing often effective for single-event PTSD, and more comprehensive, phased approaches typically necessary for CPTSD from chronic trauma. Both conditions respond to appropriate treatment, though CPTSD generally requires longer-term therapeutic work addressing the multiple layers of impact that prolonged trauma creates. Understanding which pattern describes your experience can guide decisions about seeking professional support and what approaches might be most beneficial for your specific symptoms and history.
This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm—seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
** ** **
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
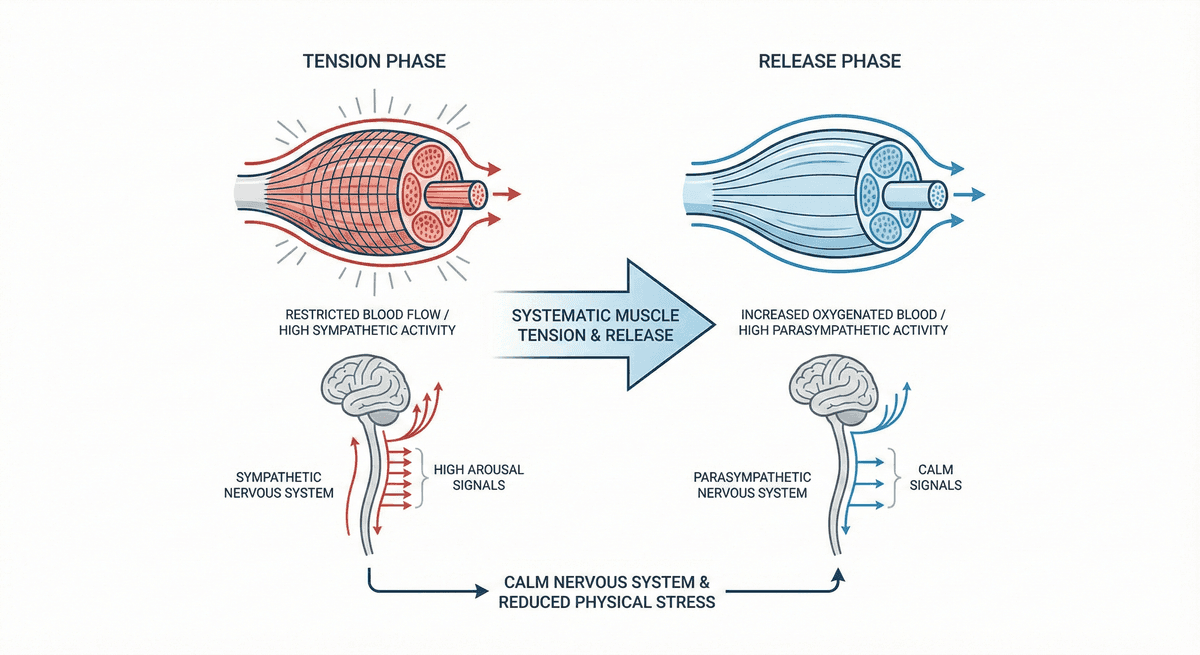
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
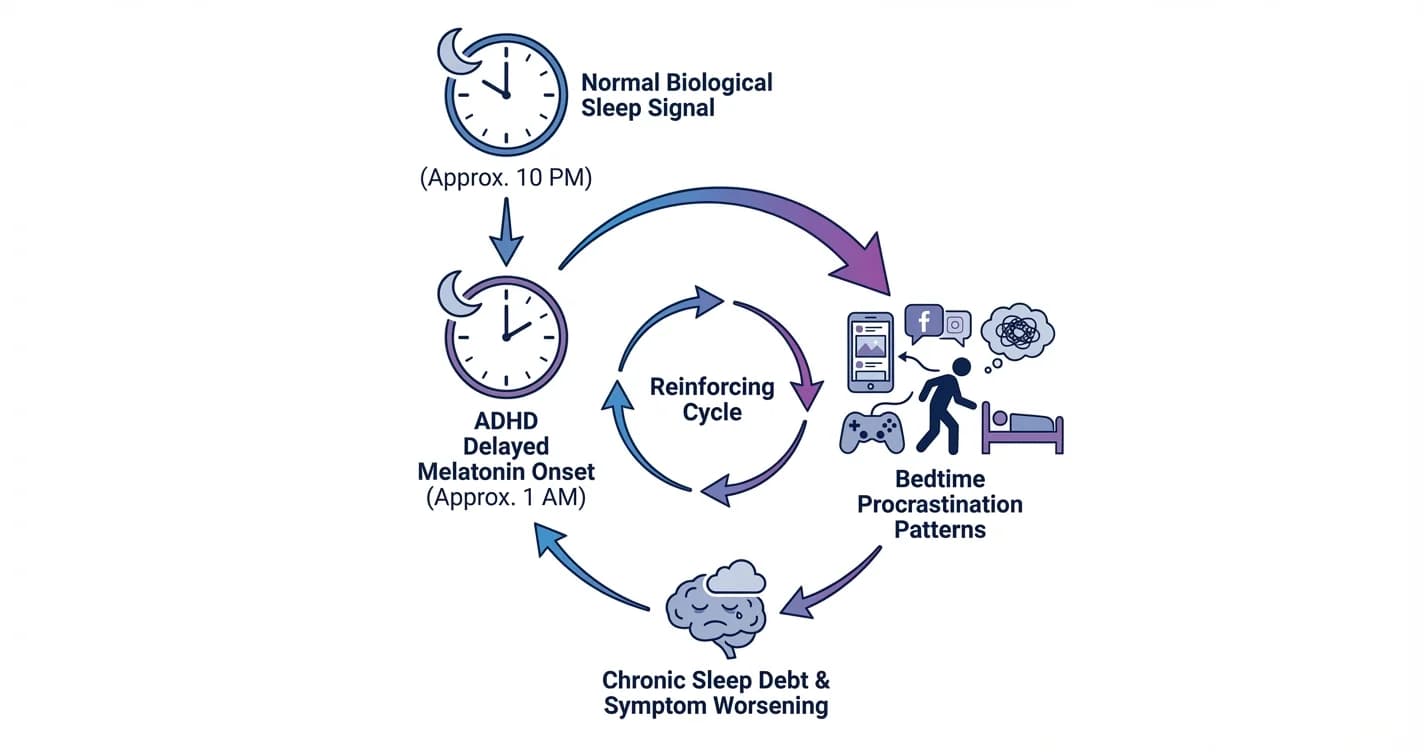
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
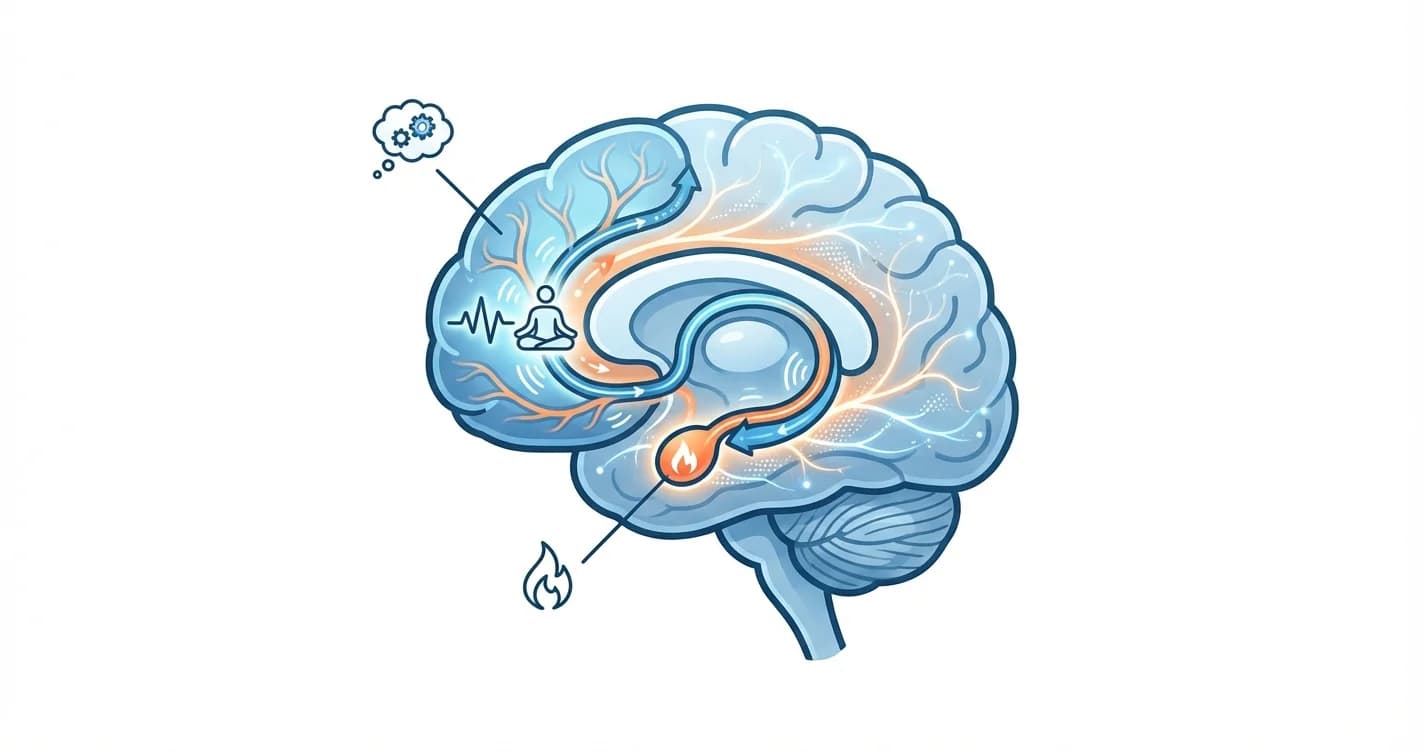
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.