EMDR Method by Francine Shapiro for Trauma Therapy Applications
The EMDR method by Francine Shapiro for trauma therapy applications has transformed how mental health professionals approach the treatment of traumatic
Key Takeaways
- The visual image representing the most disturbing part of the memory
- Negative cognitions (beliefs about oneself related to the event)
- Positive cognitions (adaptive beliefs to install)
- Emotions and their intensity
- Physical sensations associated with the memory
Introduction
The EMDR method by Francine Shapiro for trauma therapy applications has transformed how mental health professionals approach the treatment of traumatic memories and post-traumatic stress. Developed in the late 1980s, Eye Movement Desensitization and Reprocessing (EMDR) represents a departure from traditional talk therapy models, using bilateral stimulation to help the brain reprocess distressing memories. Unlike exposure-based therapies that require extensive verbal recounting of traumatic events, EMDR works through a structured eight-phase protocol that guides clients through memory reprocessing while maintaining dual attention on both the traumatic material and present-moment awareness. This article examines the practical applications of Francine Shapiro's EMDR technique in treating trauma, exploring how therapists implement this method, what research suggests about its effectiveness, and how it fits within contemporary trauma treatment approaches.
Understanding the EMDR Method by Francine Shapiro for Trauma Therapy
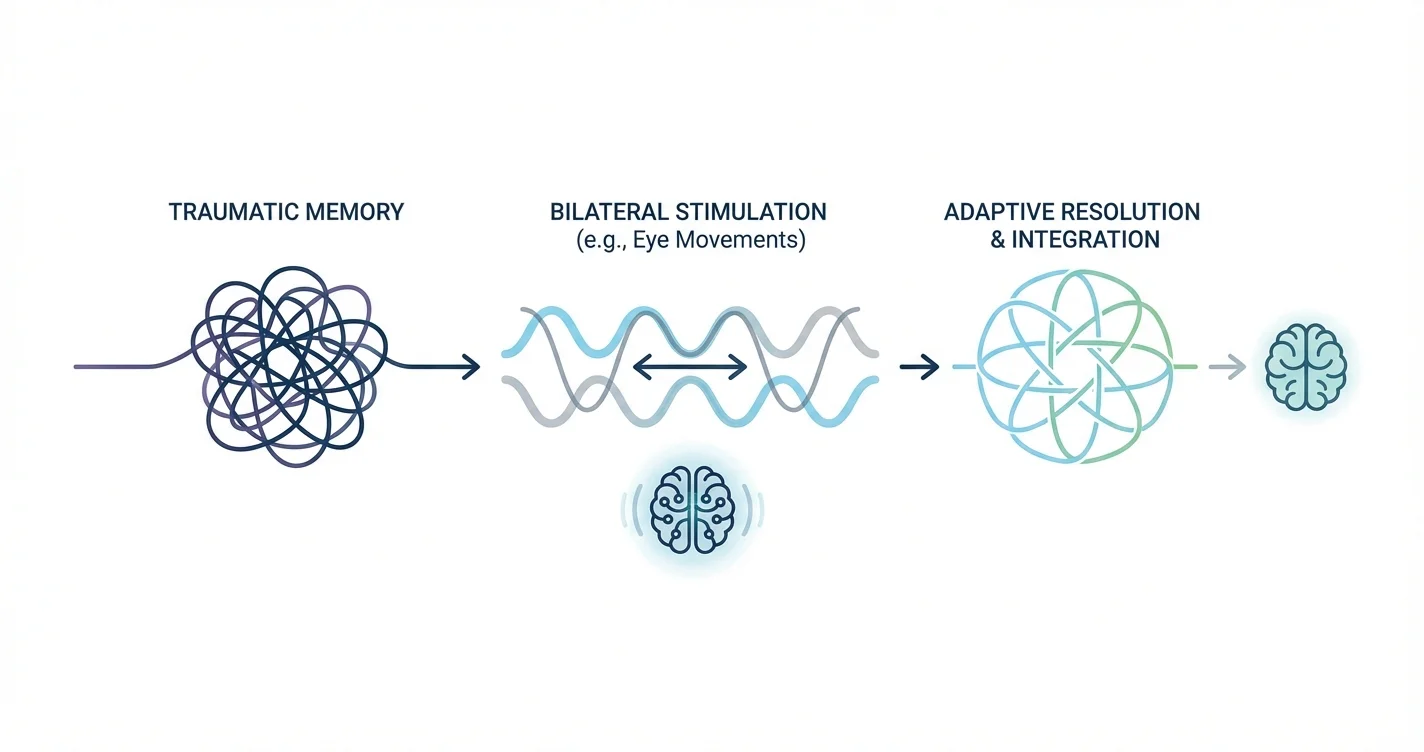
At its core, the EMDR method operates on the premise that traumatic experiences can become inadequately processed and stored in memory networks, maintaining their distressing emotional intensity. The Adaptive Information Processing model, which forms the theoretical foundation of EMDR, suggests that the brain has an innate capacity to process information toward adaptive resolution—but trauma can disrupt this natural healing mechanism.
EMDR therapy uses bilateral stimulation—typically side-to-side eye movements, though tactile taps or auditory tones may also be used—while the client briefly focuses on traumatic memories. Research suggests this dual attention process may help the brain reprocess traumatic material in a way that reduces its emotional charge and integrates it more adaptively into memory networks. The bilateral stimulation appears to facilitate the brain's information processing systems, though the exact neurobiological mechanisms remain an area of ongoing investigation.
What distinguishes EMDR from other trauma therapies is its structured approach that doesn't require extensive verbalization of traumatic details. Clients typically spend less time describing what happened and more time allowing their brain to make connections between memories, sensations, emotions, and beliefs. This can make EMDR particularly valuable for individuals who find it difficult to verbally process their trauma or who experience significant distress when asked to recount traumatic events in detail.
The Eight-Phase Protocol in Trauma Therapy Applications
Francine Shapiro's EMDR technique follows a structured eight-phase protocol that guides the therapeutic process from initial assessment through treatment completion and reevaluation:
Phase 1: History-Taking and Treatment Planning involves identifying specific traumatic memories to target, assessing client readiness for memory processing, and developing a comprehensive treatment plan. Therapists evaluate whether clients have sufficient stabilization and coping resources before beginning trauma reprocessing.
Phase 2: Preparation focuses on establishing therapeutic rapport and teaching clients self-regulation techniques they can use during and between sessions. This phase may include introducing the bilateral stimulation process and ensuring clients understand what to expect.
Phase 3: Assessment identifies specific components of the target memory, including:
- The visual image representing the most disturbing part of the memory
- Negative cognitions (beliefs about oneself related to the event)
- Positive cognitions (adaptive beliefs to install)
- Emotions and their intensity
- Physical sensations associated with the memory
Phase 4: Desensitization is where the reprocessing work occurs. The client focuses briefly on the target memory while engaging in bilateral stimulation. Sets of eye movements typically last 30-90 seconds, after which the client reports what they notice. The therapist guides this process with minimal intervention, allowing the client's brain to make its own connections and associations.
Phase 5: Installation strengthens the positive cognition identified earlier, pairing it with the original memory through additional bilateral stimulation until it feels genuinely true.
Phase 6: Body Scan checks for residual physical tension or distress related to the memory, addressing any remaining somatic components.
Phase 7: Closure ensures the client returns to a state of equilibrium before ending the session, using the stabilization techniques learned in Phase 2 if needed.
Phase 8: Reevaluation occurs at the beginning of subsequent sessions, assessing treatment progress and determining whether additional targets need attention.
This structured approach provides consistency across treatment while allowing flexibility to address individual client needs. Many therapists report that the clear protocol helps both them and their clients feel grounded during what can be emotionally challenging work.
Practical Applications Across Different Trauma Types
The application of Francine Shapiro's EMDR method extends across various trauma presentations, though implementation details may vary based on the nature and complexity of the traumatic experiences.
Single-Incident Trauma: For discrete traumatic events—such as accidents, natural disasters, or single assaults—EMDR often follows a relatively straightforward path through the eight phases. Therapists typically target the specific incident, along with any related memories that may have become associated with it. Some practitioners find that single-incident trauma may respond within a few sessions, though this varies considerably between individuals.
Complex and Developmental Trauma: When trauma occurred repeatedly over time, particularly during developmental periods, applications of EMDR require more extensive preparation and careful pacing. Therapists working with complex trauma often spend considerably more time in the preparation phase, building affect regulation skills and addressing dissociative symptoms before beginning memory reprocessing. The concept of "touchstone memories"—identifying specific representative memories from clusters of similar experiences—helps structure treatment when numerous traumatic memories exist.
Recent Trauma and Crisis Intervention: Some research suggests modified EMDR protocols may be helpful soon after traumatic events occur, potentially supporting natural recovery processes. These applications typically use abbreviated protocols and focus on supporting adaptive processing rather than formal reprocessing of memories that haven't yet consolidated.
Co-occurring Conditions: Practitioners adapting the EMDR method for clients with concurrent substance use concerns, eating disorders, or other conditions often integrate additional stabilization work and may sequence treatment to address both trauma and symptom management. The timing and pacing of trauma reprocessing becomes particularly important when clients are working on multiple recovery goals simultaneously.
Tools like Lovon.app can provide supplemental support between EMDR sessions, offering a space for clients to process emotions or reactions that may arise as memories continue to consolidate between appointments. Having accessible resources for emotional processing can be particularly valuable during active trauma work.
Evidence, Effectiveness, and Clinical Considerations
Research into EMDR therapy suggests it may be effective for treating post-traumatic stress symptoms, with multiple studies indicating outcomes comparable to other evidence-based trauma treatments. The World Health Organization and several professional organizations have recognized EMDR as an evidence-based treatment for trauma-related conditions, though research continues regarding optimal applications and mechanisms of action.
Clinical effectiveness appears to vary based on several factors:
Treatment Fidelity: Outcomes may be stronger when therapists adhere closely to the structured eight-phase protocol rather than using only portions of the method. The comprehensive approach, including adequate preparation and assessment, appears important for safety and effectiveness.
Therapist Training: EMDR training typically occurs through structured programs that include both didactic learning and supervised practice. Practitioners report that the method requires specific skills in managing abreactions (intense emotional responses during reprocessing), pacing treatment appropriately, and recognizing when additional stabilization is needed.
Client Readiness: Not all clients are appropriate candidates for trauma reprocessing at any given time. Contraindications may include active psychosis, severe dissociative disorders without adequate management strategies, significant self-harm risk, or insufficient affect regulation skills. Thorough assessment helps determine appropriate timing for introducing memory reprocessing work.
Treatment Dose: The number of sessions needed varies considerably based on trauma complexity, individual processing styles, and co-occurring factors. Single-incident trauma may show significant improvement within several sessions, while complex developmental trauma typically requires extended treatment.
It's important to note that EMDR is one of several evidence-based approaches to trauma treatment. Some individuals may respond better to other modalities such as prolonged exposure therapy, cognitive processing therapy, or somatic approaches. The choice of treatment approach should consider individual preferences, therapist expertise, and specific clinical presentations.
Integration with Contemporary Trauma Treatment
The EMDR method by Francine Shapiro exists within a broader landscape of trauma therapy applications, and many practitioners integrate elements from multiple approaches to address individual client needs comprehensively.
Attachment-Focused Adaptations: Some therapists integrate attachment theory and relational focus into EMDR work, particularly when treating developmental trauma. This might include targeting attachment-related beliefs and incorporating the therapeutic relationship as a resource during reprocessing.
Somatic Integration: Given that trauma often manifests in physical symptoms and body-based experiences, many EMDR practitioners emphasize the body scan phase and integrate somatic awareness throughout treatment. This recognizes that trauma processing involves not just cognitive and emotional work but also releasing held patterns in the nervous system.
Preparation Phase Enhancements: Contemporary applications often expand the preparation phase to include more extensive work on window of tolerance, polyvagal-informed regulation strategies, and parts work for clients with dissociative presentations. This reflects growing understanding that adequate stabilization supports more effective and safer trauma reprocessing.
Cultural Considerations: Practitioners adapting EMDR across different cultural contexts attend to how trauma is understood, expressed, and processed in various communities. This includes considering collective versus individual trauma, the role of spirituality, and culturally relevant resources and metaphors.
Between formal therapy sessions, having accessible support can help clients manage emotions or insights that emerge during the integration period. Resources like Lovon.app provide on-demand access to process reactions and maintain emotional regulation as memory reconsolidation continues between appointments.
When to Seek Professional Help
If you're experiencing symptoms of trauma—including intrusive memories, avoidance of reminders, heightened reactivity, negative changes in mood or thinking, or functional impairment in daily life—seeking evaluation from a mental health professional is an important step. Trauma specialists, including licensed therapists trained in EMDR, can assess whether this approach might be appropriate for your situation.
Professional help becomes particularly important when:
- Trauma symptoms interfere with work, relationships, or daily functioning
- You experience flashbacks or dissociative episodes
- Avoidance patterns significantly limit your life
- You have thoughts of self-harm or suicide
- Previous self-help strategies haven't provided adequate relief
Licensed clinical social workers, psychologists, professional counselors, and other mental health professionals with specialized EMDR training can provide this treatment. Many therapists list their specific training and trauma specializations in their professional profiles, making it easier to identify providers with relevant expertise.
Conclusion
The EMDR method by Francine Shapiro for trauma therapy applications offers a structured, evidence-informed approach to processing traumatic memories that differs significantly from traditional talk therapy models. Through its eight-phase protocol and use of bilateral stimulation, EMDR helps individuals reprocess distressing memories in ways that reduce their emotional intensity and integrate them more adaptively. While research suggests EMDR can be effective for many individuals experiencing trauma-related symptoms, it represents one valuable tool within a comprehensive trauma treatment toolkit rather than a universal solution.
Understanding how Francine Shapiro's EMDR works for trauma therapy—including its structured phases, bilateral stimulation component, and emphasis on the brain's natural information processing—can help individuals make informed decisions about their treatment options. Whether EMDR becomes part of your healing journey depends on multiple factors including the nature of your experiences, your current stability and resources, and your preferences for how to approach recovery work. Consulting with trauma-informed mental health professionals can help you determine whether this approach aligns with your needs and circumstances.
Disclaimer: This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm — seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
How AI Support Helps You Heal
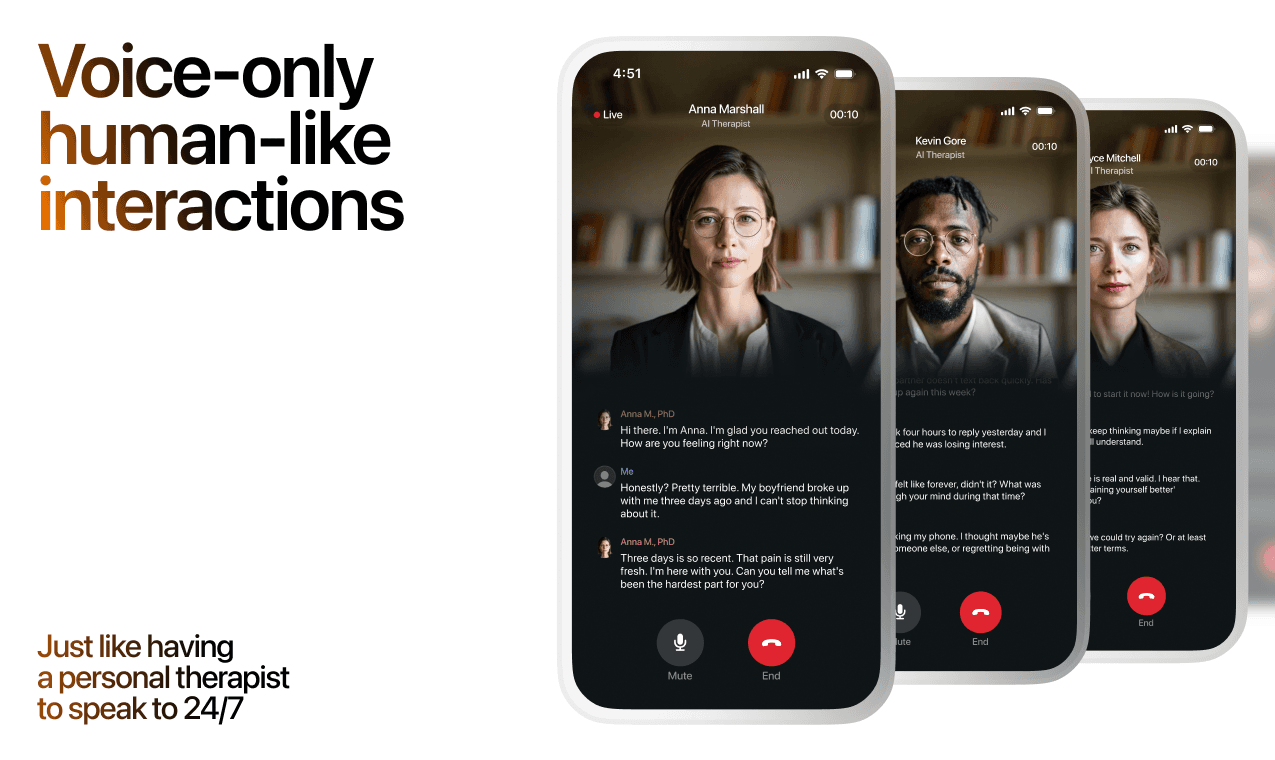
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
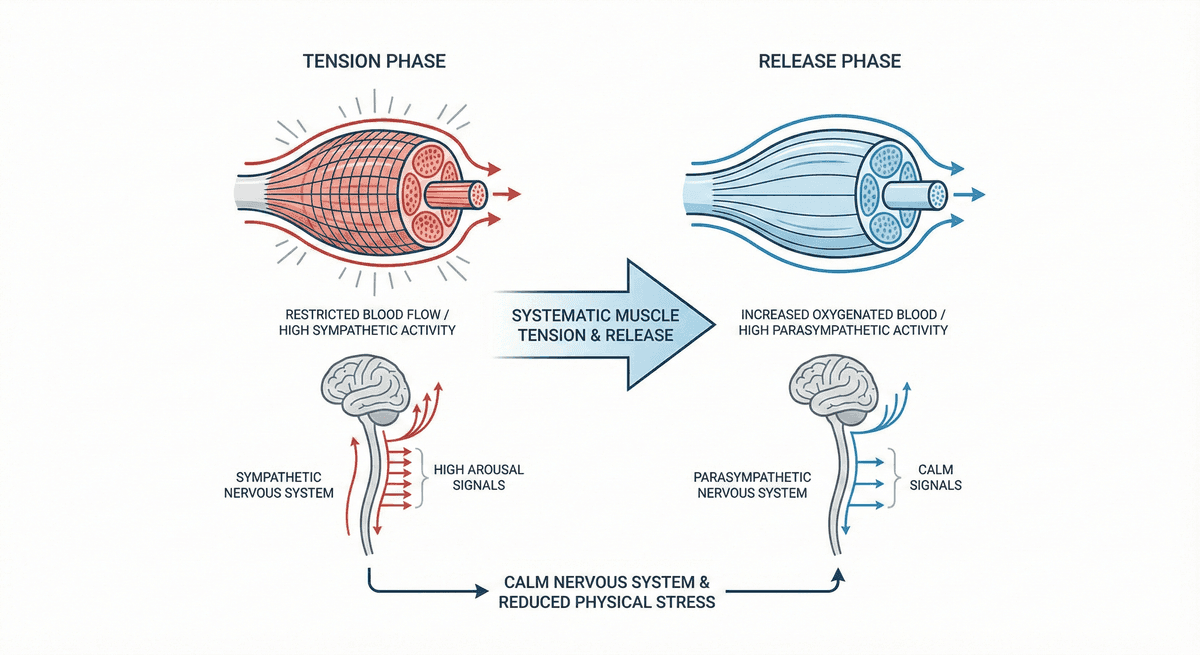
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
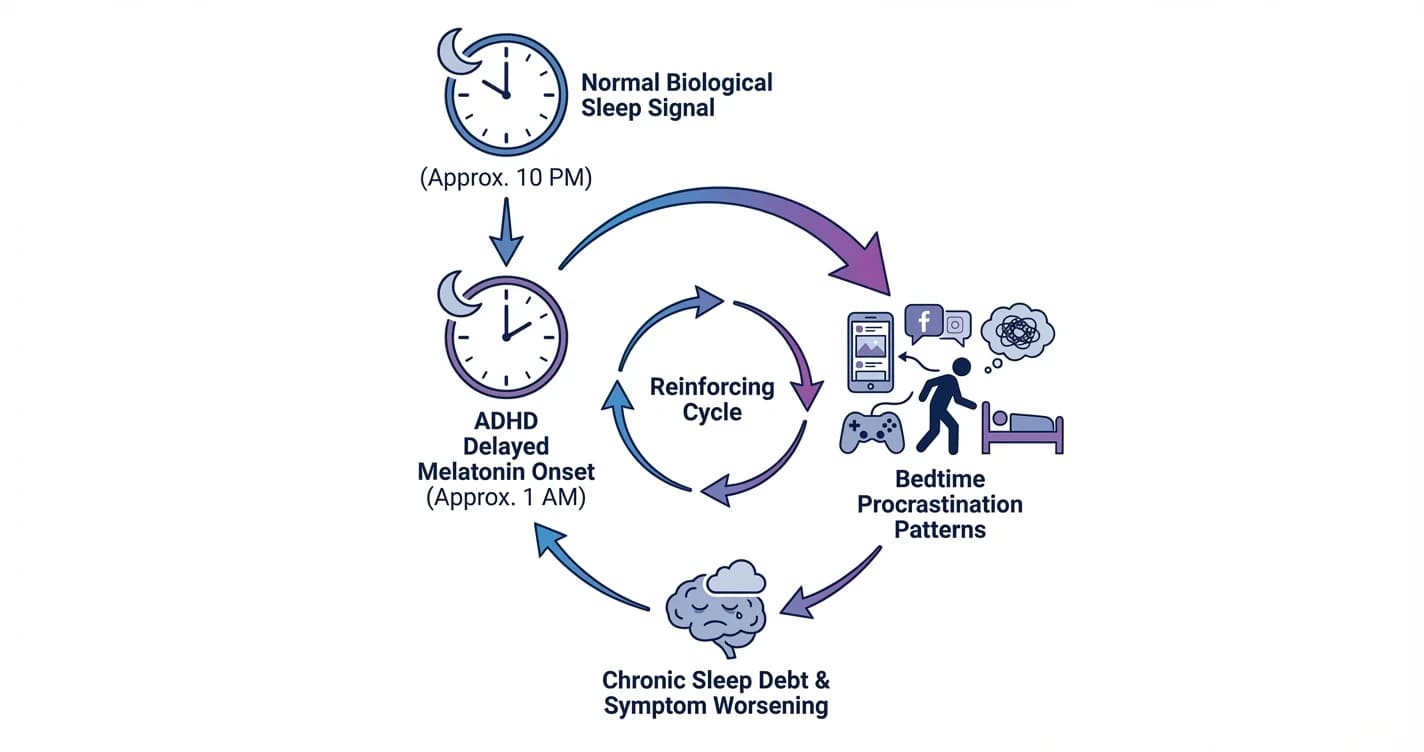
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.