PTSD Four Symptom Categories: Intrusive Memories vs Flashbacks Distinction
Post-Traumatic Stress Disorder manifests through complex symptom patterns that clinicians organize into four distinct categories for diagnostic purposes.
Key Takeaways
- Persistent negative beliefs about oneself, others, or the world
- Distorted blame of self or others regarding trauma causes or consequences
- Persistent negative emotional states such as fear, horror, anger, guilt, or shame
- Diminished interest in significant activities
- Feelings of detachment from others
Introduction
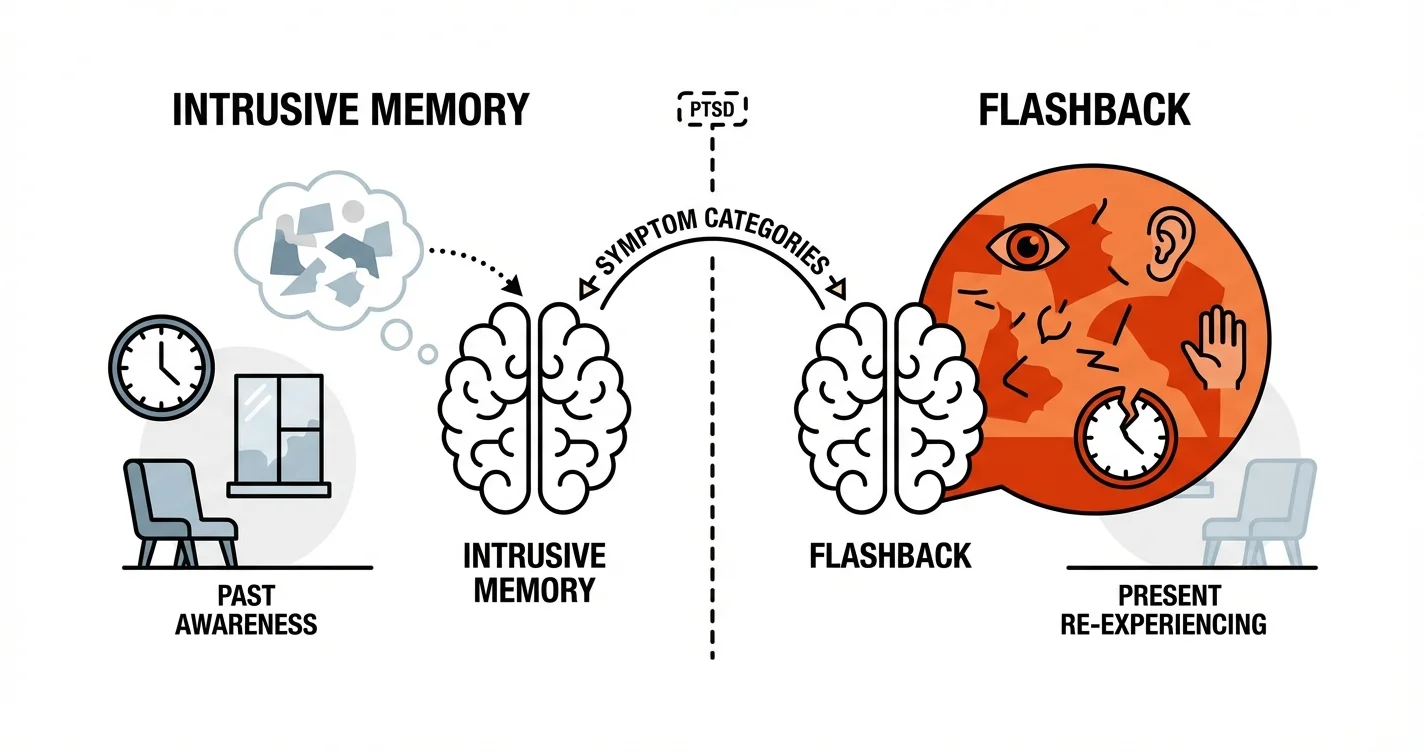
Post-Traumatic Stress Disorder manifests through complex symptom patterns that clinicians organize into four distinct categories for diagnostic purposes. Within these PTSD four symptom categories, intrusive memories and flashbacks represent two related but fundamentally different experiences that individuals often confuse. While both involve unwanted recollections of traumatic events, the nature of how these memories intrude into consciousness differs significantly in terms of sensory intensity, temporal awareness, and psychological impact. Understanding the intrusive memories vs flashbacks distinction is essential for accurate symptom recognition, effective treatment planning, and helping individuals validate their experiences. This article explores the clinical framework that distinguishes these phenomena and provides practical guidance for recognizing and responding to each type of intrusive experience.
The Four Symptom Categories of PTSD
The diagnostic framework for PTSD organizes symptoms into four primary clusters that help clinicians assess and understand the full scope of post-traumatic responses. These categories reflect how trauma impacts multiple aspects of psychological functioning rather than producing a single uniform response.
The first category, intrusion symptoms, encompasses various ways traumatic memories force themselves into conscious awareness without invitation. This includes intrusive memories, flashbacks, nightmares, and intense psychological distress when exposed to trauma reminders. The second category involves persistent avoidance of trauma-associated stimuli—both external reminders and internal thoughts or feelings connected to the event.
The third category addresses negative alterations in cognitions and mood, including:
- Persistent negative beliefs about oneself, others, or the world
- Distorted blame of self or others regarding trauma causes or consequences
- Persistent negative emotional states such as fear, horror, anger, guilt, or shame
- Diminished interest in significant activities
- Feelings of detachment from others
- Persistent inability to experience positive emotions
The fourth category involves marked alterations in arousal and reactivity, such as hypervigilance, exaggerated startle response, concentration difficulties, sleep disturbances, and irritable or aggressive behavior. Research indicates that individuals rarely experience symptoms from only one category—the interaction between symptom clusters often determines the overall severity and functional impact of PTSD.
Within the intrusion category, the distinction between intrusive memories and flashbacks represents a spectrum of re-experiencing phenomena rather than completely separate experiences. Both stem from how traumatic memories become encoded and stored differently than ordinary memories, but they manifest with distinct characteristics that have important implications for treatment approaches.
Defining Intrusive Memories Within PTSD Four Symptom Categories
Intrusive memories represent unwanted, involuntary recollections of traumatic events that enter conscious awareness suddenly and without deliberate effort to remember. These memories maintain a quality of "pastness"—the person experiencing them recognizes they are remembering something that happened previously, even though the memory feels unwanted and distressing.
Clinical observations suggest that intrusive memories typically involve specific sensory fragments rather than complete narrative sequences. A person might suddenly recall the smell of smoke, the sound of impact, or a visual image of a particular moment during the trauma. These sensory fragments often appear more vivid and emotionally charged than ordinary memories, carrying the affective intensity of the original experience despite the person's awareness that they are in the present moment.
The involuntary nature distinguishes intrusive memories from deliberate recollection. While someone might choose to talk about their traumatic experience in therapy, intrusive memories arrive without invitation—triggered by environmental cues, appearing during quiet moments, or emerging seemingly without any identifiable prompt. Studies indicate that these memories may represent inadequately processed trauma material that hasn't been fully integrated into autobiographical memory networks.
Unlike flashbacks, intrusive memories occur while the person maintains dual awareness: they simultaneously experience the memory's emotional and sensory content while remaining oriented to their current environment and time. This dual awareness means that despite the memory's distressing nature, the person recognizes they are safe in the present moment, even if their body responds with anxiety symptoms.
The frequency and intensity of intrusive memories often fluctuate based on stress levels, exposure to trauma reminders, and proximity to trauma anniversaries. Some people experience multiple intrusions daily, while others may have periods of relative calm interrupted by occasional intrusive recollections. The content typically remains stable over time, with the same fragments recurring rather than new details emerging, which distinguishes trauma-related intrusions from other memory phenomena.
Understanding Flashbacks: The Intrusive Memories vs Flashbacks Distinction
Flashbacks represent a more immersive form of re-experiencing within the PTSD four symptom categories, characterized by a temporary loss of orientation to present circumstances. During a flashback, the boundary between past and present becomes permeable—the person doesn't simply remember the trauma but experiences a compelling sense that it is happening again in the current moment.
The defining feature of flashbacks involves this disruption of temporal orientation. While intrusive memories carry a quality of "remembering when," flashbacks create an experience of "happening now." This distinction isn't merely semantic—it reflects different neurobiological processes and requires different intervention approaches. The person may lose awareness of their current surroundings partially or completely, responding to the traumatic memory as though it represents immediate reality.
Flashbacks exist on a spectrum of intensity and duration. Some last only seconds, creating a brief moment of disorientation before the person reorients to the present. Others may continue for minutes, with the individual behaving as though they are back in the traumatic situation—ducking for cover, attempting to flee, or freezing in place. The most intense flashbacks involve full sensory immersion across multiple modalities: visual, auditory, olfactory, tactile, and kinesthetic sensations that recreate the trauma environment.
Neuroimaging studies suggest that during flashbacks, brain activation patterns differ from those during ordinary memory recall. The areas involved in contextualizing memories as past events may show reduced activity, while sensory and emotional processing regions demonstrate heightened activation. This pattern may explain why flashbacks feel more real and immediate than typical memories.
The intrusive memories vs flashbacks distinction also involves differences in sensory completeness. Intrusive memories often involve specific fragments—a particular image, sound, or sensation. Flashbacks tend to engage multiple sensory systems simultaneously, creating a more complete perceptual experience that mimics the original trauma environment. This multisensory integration contributes to the flashback's convincing quality and the difficulty people have recognizing them as memories rather than current events.
Environmental triggers play a prominent role in flashback onset. Sensory cues that resemble aspects of the trauma—certain smells, sounds, lighting conditions, or physical sensations—can precipitate flashbacks in susceptible individuals. However, flashbacks can also occur without obvious external triggers, emerging during sleep transitions, periods of relaxation, or states of heightened stress when cognitive resources for maintaining present-moment orientation become depleted.
Recognizing the Differences in Daily Life
Understanding how intrusive memories and flashbacks manifest differently in everyday situations helps individuals and their support networks respond appropriately. These distinctions have practical implications for safety, functioning, and treatment approach.
When experiencing an intrusive memory, a person typically remains capable of continued interaction with their environment, though they may appear distracted or emotionally affected. They might pause mid-conversation, seem momentarily absent, or show signs of distress such as tension or tearfulness, but they generally maintain awareness of where they are and whom they're with. Communication remains possible—they can usually acknowledge the intrusion if asked and can often be redirected through conversation or gentle grounding techniques.
During a flashback, observable behavior changes more dramatically. The person may:
- Stop responding to their name or to questions
- Exhibit protective behaviors such as covering their head, crouching, or attempting to hide
- Display intense fear responses disproportionate to the current environment
- Make statements indicating they believe the trauma is occurring now ("It's happening again," "They're coming")
- Show dilated pupils, rapid breathing, or other pronounced physiological arousal
- Become temporarily unaware of people or objects in their immediate surroundings
The recovery pattern differs as well. After an intrusive memory, the person typically returns to baseline functioning relatively quickly once they redirect attention or use coping strategies. Following a flashback, there's often a period of disorientation, confusion, or exhaustion as the person reorients to present reality. They may feel embarrassed, frightened by the loss of control, or physically depleted from the intense physiological activation.
For those supporting someone with PTSD, recognizing whether the person is experiencing an intrusive memory or a flashback guides appropriate response. During intrusive memories, gentle conversation, validation of feelings, and helping redirect attention often suffice. During flashbacks, safety becomes paramount—ensuring the person doesn't injure themselves, using a calm voice to provide orientation information ("You're safe, it's [year], you're in [location]"), and avoiding sudden movements or touches that might be misinterpreted as threats.
Tools like Lovon.app can help individuals process these experiences between therapy sessions, providing on-demand support to talk through what happened, identify triggers, and develop personalized coping strategies. When you notice patterns in when intrusive memories or flashbacks occur, discussing these observations with a trained listener—whether human or AI-assisted—can help you prepare for and manage future episodes more effectively.
Clinical Implications and Treatment Approaches
The distinction between intrusive memories and flashbacks within the PTSD four symptom categories influences treatment planning and therapeutic techniques. While both respond to evidence-based PTSD treatments, specific interventions may be emphasized differently depending on which re-experiencing phenomena predominate.
Trauma-focused cognitive behavioral therapy approaches help address both intrusive memories and flashbacks by facilitating trauma memory processing. These methods work by helping individuals create more complete, organized narratives of traumatic events, which may reduce memory fragmentation and intrusive recurrence. For intrusive memories specifically, techniques that strengthen contextual information—reinforcing that the trauma occurred in the past and is no longer happening—can reduce their emotional intensity and frequency.
For flashbacks, interventions emphasizing grounding and present-moment awareness become particularly important. Grounding techniques that engage multiple sensory systems help restore orientation to current reality during flashback episodes. These might include identifying five things you can see, four you can touch, three you can hear, two you can smell, and one you can taste—progressively anchoring awareness in the present environment.
Eye Movement Desensitization and Reprocessing (EMDR) has shown effectiveness for both intrusive memories and flashbacks by facilitating adaptive processing of trauma memories. The bilateral stimulation component may help integrate fragmented sensory memories into more cohesive narratives with appropriate contextual markers, reducing both intrusive recollections and dissociative re-experiencing.
Medication approaches may complement psychotherapy, particularly when intrusive symptoms significantly impair functioning or interfere with engagement in trauma-focused treatment. For individuals whose symptoms make daily functioning difficult, discussing medication options with a prescriber can be an important component of comprehensive care.
Some people find that working with accessible support tools between therapy sessions helps maintain momentum in recovery. Platforms like Lovon.app allow individuals to process difficult moments when they arise rather than waiting until the next scheduled appointment, which can be particularly helpful when intrusive symptoms intensify or new triggers are identified.
The intrusive memories vs flashbacks distinction also matters for treatment sequencing. When flashbacks occur frequently and create safety concerns or severe distress, stabilization and grounding skills often receive initial focus before proceeding to direct trauma processing. In contrast, when intrusive memories predominate without dissociative re-experiencing, earlier introduction of trauma-focused work may be appropriate.
Research suggests that treatment outcomes improve when interventions address the specific characteristics of an individual's symptom presentation rather than applying a one-size-fits-all approach. This personalization requires ongoing assessment of symptom patterns and adjustment of therapeutic techniques as treatment progresses and symptoms evolve.
When to Seek Professional Help
While understanding the PTSD four symptom categories and the intrusive memories vs flashbacks distinction provides valuable knowledge, certain signs indicate professional evaluation and treatment are necessary.
Seek professional help if you experience:
- Flashbacks or intrusive memories that occur frequently enough to interfere with work, relationships, or daily activities
- Increasing avoidance of people, places, or activities due to fear of triggering intrusive symptoms
- Inability to function normally for extended periods following flashbacks
- Intrusive symptoms that persist for more than a month after a traumatic event
- Self-harm thoughts or behaviors related to trauma symptoms
- Substance use to manage intrusive memories or flashbacks
- Significant sleep disruption from nightmares or hypervigilance
- Relationship difficulties stemming from trauma symptoms
Mental health professionals specializing in trauma—including psychologists, psychiatrists, licensed clinical social workers, and counselors with trauma training—can provide comprehensive assessment and evidence-based treatment. PTSD responds well to treatment, and early intervention often leads to better outcomes than waiting until symptoms become entrenched.
For individuals already in treatment, discussing changes in symptom patterns with your therapist helps ensure your treatment plan remains appropriate. If intrusive memories evolve into flashbacks, or if new triggers emerge, adjusting therapeutic approaches may optimize progress.
Conclusion
The distinction between intrusive memories and flashbacks within the PTSD four symptom categories represents more than academic classification—it reflects meaningful differences in how trauma impacts consciousness, orientation, and functioning. Intrusive memories involve unwanted but recognized recollections of past trauma, maintaining awareness that these are memories rather than current reality. Flashbacks create more immersive re-experiencing where the boundary between past and present temporarily dissolves, leading to responses as though the trauma is occurring again.
Recognizing the intrusive memories vs flashbacks distinction enables more accurate symptom monitoring, appropriate support responses, and targeted treatment planning. Both phenomena respond to evidence-based trauma treatments, though specific techniques may be emphasized differently depending on symptom presentation. Whether working with a therapist, using between-session support resources, or developing personal coping strategies, understanding these differences empowers more effective management of post-traumatic symptoms.
If you're experiencing intrusive memories or flashbacks that interfere with your quality of life, professional evaluation provides the foundation for recovery. PTSD symptoms can improve significantly with appropriate treatment, and seeking help represents a crucial step toward reclaiming your life from trauma's impact.
Disclaimer: This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm—seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
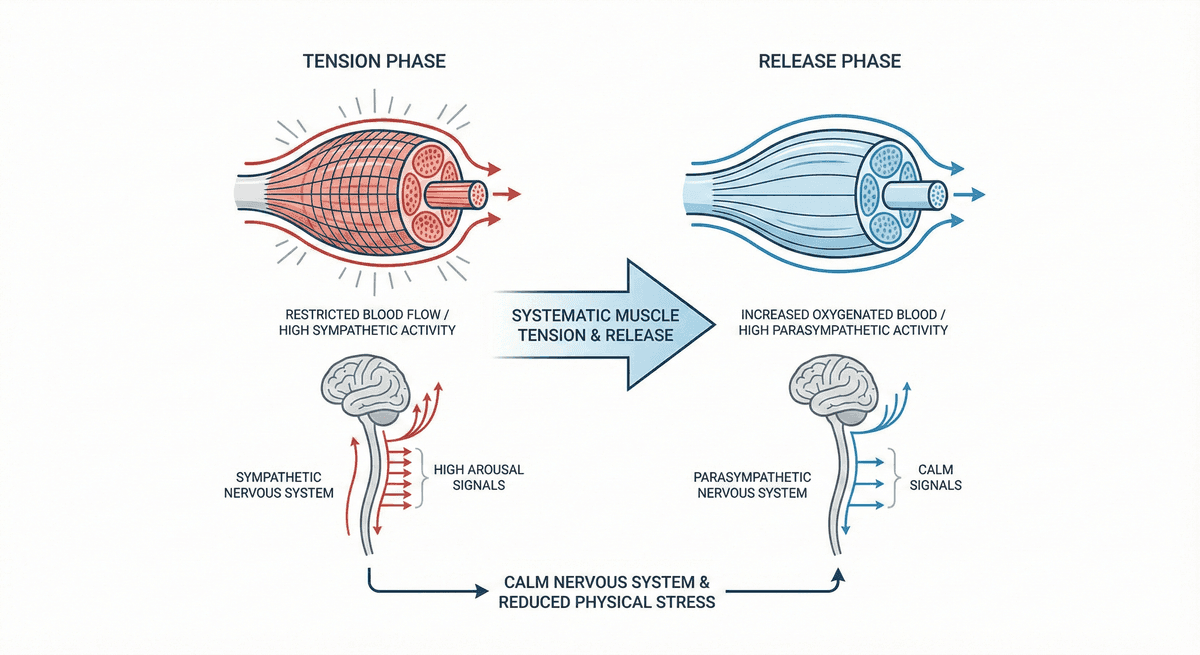
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
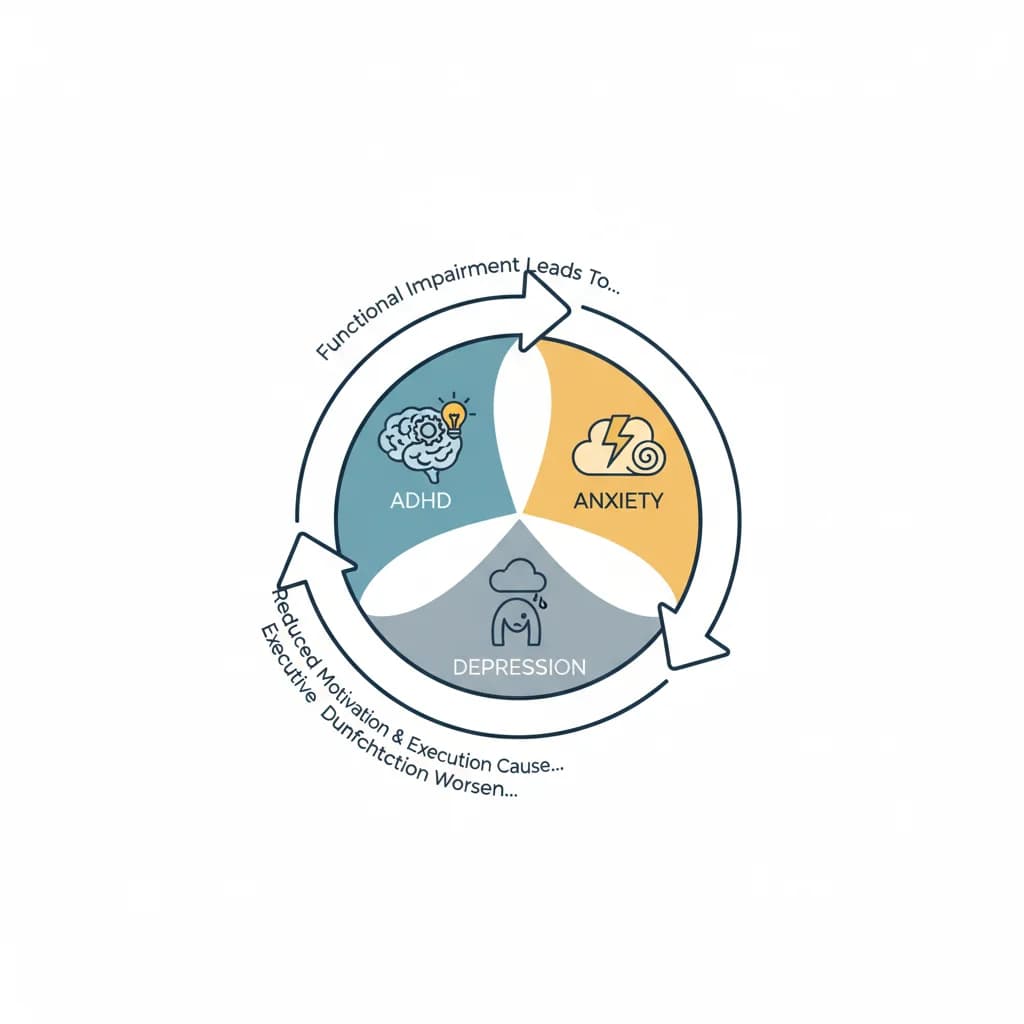
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
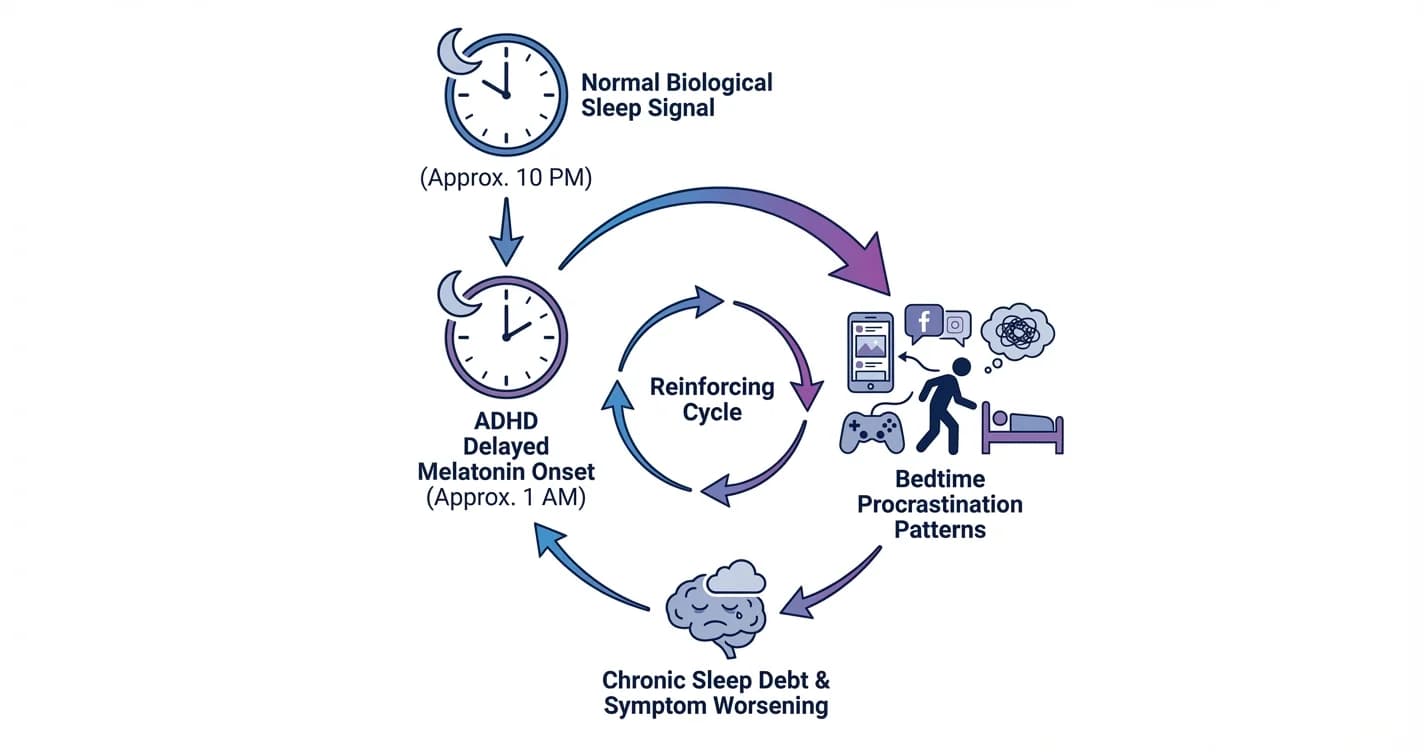
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.