CPTSD — Affect Regulation Difficulties and Self-Concept Disturbances Beyond PTSD
Complex Post-Traumatic Stress Disorder (CPTSD) represents a significant expansion beyond traditional PTSD, characterized by profound affect regulation
Key Takeaways
- Difficulty identifying and labeling emotional states (alexithymia)
- Rapid emotional escalation with limited capacity to self-soothe
- Emotional numbing or dissociation as primary coping mechanisms
- Alternating between emotional flooding and complete shutdown
- Limited access to a middle range of emotional experience
Introduction
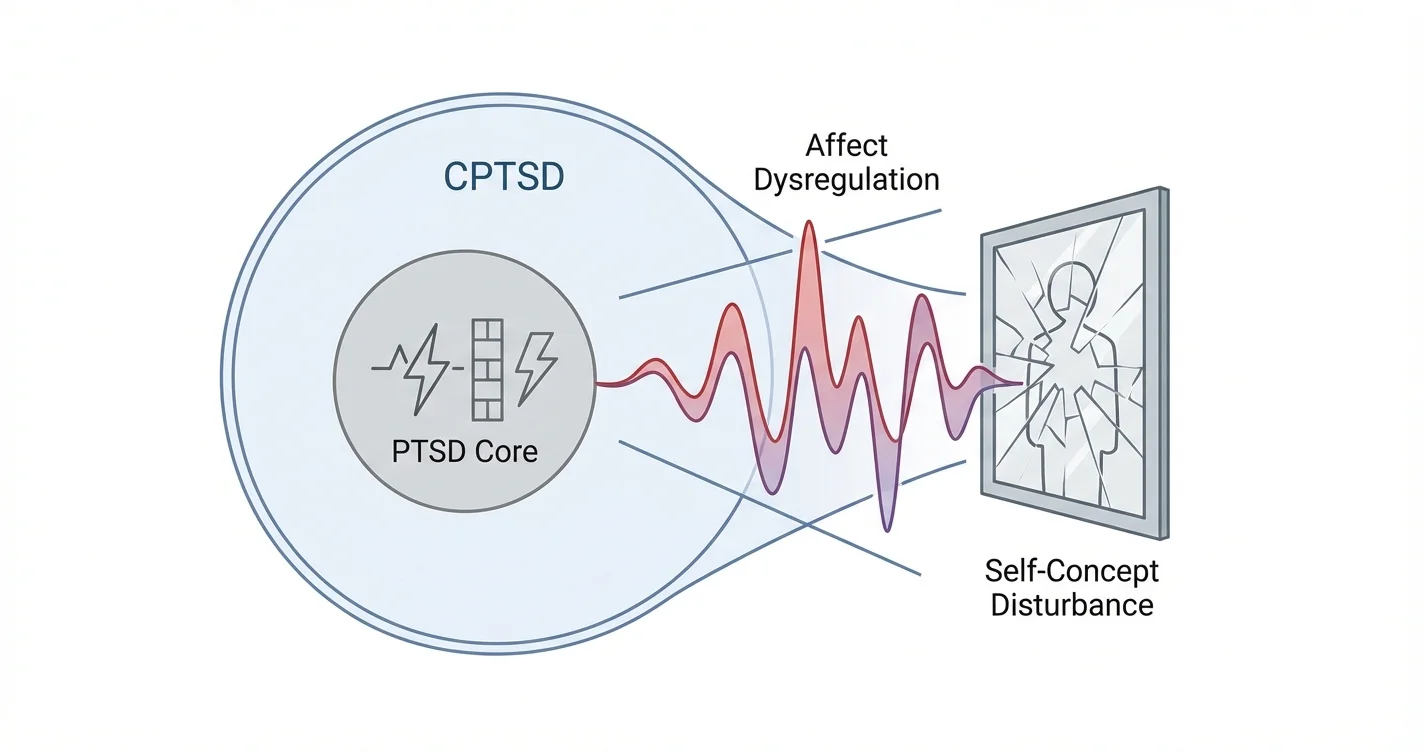
Complex Post-Traumatic Stress Disorder (CPTSD) represents a significant expansion beyond traditional PTSD, characterized by profound affect regulation difficulties and self-concept disturbances that fundamentally alter how individuals experience themselves and manage emotions. While PTSD typically develops from discrete traumatic events, CPTSD emerges from prolonged, repeated trauma—often during developmental periods—creating additional symptom clusters that complicate recovery and daily functioning. The distinction between these conditions is not merely academic; it has substantial implications for treatment approaches and understanding the lived experience of trauma survivors. Research from trauma psychology indicates that individuals with CPTSD face challenges in emotional regulation and identity coherence that extend far beyond the core PTSD symptoms of intrusion, avoidance, and hyperarousal.
Understanding Affect Regulation Difficulties in CPTSD
Affect regulation refers to the capacity to modulate emotional responses appropriately to situational demands—maintaining emotional equilibrium while experiencing and expressing feelings in adaptive ways. In CPTSD, affect regulation difficulties and self-concept disturbances beyond PTSD create a pervasive pattern of emotional dysregulation that differs qualitatively from standard PTSD presentations.
Individuals with complex PTSD emotional regulation problems experience several distinctive patterns. Emotional responses may be disproportionate to triggering events, with seemingly minor stressors producing overwhelming emotional reactions. This hyperreactivity stems from a nervous system conditioned by prolonged threat exposure, where the capacity to calibrate emotional responses becomes compromised. Unlike PTSD, where emotional dysregulation typically connects to specific trauma reminders, CPTSD involves more generalized difficulty managing emotional states across diverse situations.
Studies indicate that these regulation problems manifest in several ways:
- Difficulty identifying and labeling emotional states (alexithymia)
- Rapid emotional escalation with limited capacity to self-soothe
- Emotional numbing or dissociation as primary coping mechanisms
- Alternating between emotional flooding and complete shutdown
- Limited access to a middle range of emotional experience
The chronic nature of developmental or relational trauma interferes with the natural acquisition of affect regulation skills during critical periods. When caregivers who should provide co-regulation are themselves sources of threat or unpredictability, children cannot internalize healthy emotional management strategies. This developmental disruption creates lasting vulnerabilities that persist into adulthood.
Self-Concept Disturbances That Distinguish CPTSD from PTSD
Self-concept disturbances represent perhaps the most defining feature separating CPTSD from standard PTSD. While PTSD may involve negative cognitions about oneself related to the traumatic event, complex trauma fundamentally disrupts core identity formation and self-perception.
Research suggests that self-concept disturbances in CPTSD include persistent negative self-evaluation, pervasive shame, and a fragmented sense of identity. Survivors often describe feeling fundamentally flawed, damaged, or unworthy—not as a response to specific trauma memories, but as a core aspect of how they experience themselves. This differs markedly from PTSD, where self-perception problems typically relate directly to trauma-specific guilt or responsibility.
The self-concept issues in CPTSD manifest through several patterns:
- Pervasive shame and worthlessness: A deep-seated belief in being fundamentally defective or unlovable, extending beyond trauma-related guilt
- Identity confusion: Difficulty maintaining a coherent sense of self across time and contexts, sometimes described as feeling like "different people" in different situations
- Self-as-victim identity: An organizing life narrative centered on victimhood that becomes difficult to revise even with recovery progress
- Contaminated self-perception: Feeling permanently altered or "tainted" by trauma experiences in ways that cannot be remedied
These disturbances often trace to relational trauma where the perpetrator was a caregiver or attachment figure. When abuse or neglect occurs within relationships that should provide safety and identity formation, the developing self incorporates traumatic relational patterns as core self-understanding. The child may internalize messages that they caused the abuse, deserved mistreatment, or are inherently unlovable—beliefs that become foundational to identity rather than event-specific cognitions.
How CPTSD Differs from PTSD in Emotional and Interpersonal Functioning
Understanding how CPTSD differs from PTSD in terms of affect regulation and self-concept disturbances requires examining their impact on interpersonal relationships and daily functioning. Complex trauma additional symptoms create patterns that significantly complicate social connection and emotional intimacy.
Individuals with CPTSD frequently experience relationship difficulties that stem directly from affect regulation and self-concept problems. Emotional dysregulation may manifest as intense, unstable relationships characterized by fears of abandonment, difficulty trusting others, and hypersensitivity to perceived rejection. The self-concept disturbances contribute to relationship patterns where individuals struggle to maintain boundaries, may tolerate mistreatment due to internalized worthlessness, or alternate between desperate connection-seeking and defensive withdrawal.
Clinical experience suggests several distinguishing interpersonal features:
- Difficulty establishing and maintaining appropriate interpersonal boundaries
- Patterns of reenacting traumatic relationship dynamics
- Extreme sensitivity to interpersonal cues suggesting rejection or criticism
- Challenges with emotional intimacy due to affect dysregulation and shame
- Tendency toward idealization and devaluation of others
These patterns reflect what trauma specialists describe as "relational trauma"—where the trauma itself occurred within attachment relationships, fundamentally shaping how individuals approach connection. For someone with standard PTSD from a single traumatic event like a car accident, relationships may be affected by avoidance or hypervigilance, but the core capacity for healthy attachment typically remains intact. In CPTSD, the attachment system itself may be organized around traumatic expectations.
Tools like Lovon.app can provide accessible support for processing these complex relational and emotional patterns between therapy sessions, offering on-demand conversation when overwhelming emotions or relationship difficulties arise.
CPTSD Specific Features: Treatment Implications and Recovery Considerations
The CPTSD specific features of emotional dysregulation and identity disturbances require treatment approaches that extend beyond standard PTSD interventions. While trauma-focused therapies remain important, addressing complex trauma requires additional focus on affect regulation skill-building and identity reconstruction.
Effective treatment for CPTSD typically involves a phased approach. Initial phases prioritize safety and stabilization, with substantial emphasis on developing affect regulation capacities before intensive trauma processing. This differs from some PTSD protocols that move relatively quickly to trauma-focused work. For individuals with severe affect regulation difficulties, premature trauma processing may trigger overwhelming emotional responses that reinforce rather than resolve traumatic patterns.
Treatment components that address the distinctive features of CPTSD include:
- Affect regulation skill development: Techniques for identifying emotions, tolerating distress, and modulating emotional intensity
- Identity work: Exploring and reconstructing self-narratives that integrate trauma history without organizing identity around victimhood
- Relational repair: Addressing interpersonal patterns and attachment difficulties through therapeutic relationship and interpersonal skills training
- Shame reduction: Specific interventions targeting pervasive shame and self-blame distinct from trauma-specific guilt
- Somatic approaches: Body-based interventions recognizing that affect dysregulation and trauma responses are stored physiologically
Recovery from CPTSD is often described as a longer, more complex process than PTSD treatment, reflecting the pervasive nature of affect regulation and self-concept difficulties. Progress may be non-linear, with gains in one area (such as emotional regulation) revealing previously obscured challenges in another (such as relationship patterns). This complexity requires sustained therapeutic support and realistic expectations about recovery timelines.
Between therapy sessions or during particularly difficult periods, accessible resources can help maintain progress. Platforms like Lovon.app offer on-demand support for processing emotional experiences and relationship challenges as they arise, providing a space to talk through difficulties when traditional therapy isn't immediately available.
When to Seek Professional Help
If you recognize patterns of severe emotional dysregulation—such as frequent emotional flooding, persistent dissociation, or self-harming behaviors—professional support is essential. Similarly, if self-concept disturbances significantly impair your daily functioning, relationships, or quality of life, specialized trauma therapy can provide crucial assistance.
Therapists specializing in complex trauma, particularly those trained in approaches like EMDR, Sensorimotor Psychotherapy, or Dialectical Behavior Therapy adapted for trauma, can offer evidence-informed treatment addressing both affect regulation difficulties and identity disturbances. Psychiatrists may also help assess whether medication could support emotional regulation while engaging in trauma-focused therapy.
Signs that professional help is particularly important include:
- Emotional responses that feel completely unmanageable or lead to dangerous behaviors
- Persistent dissociation interfering with memory, identity, or daily functioning
- Relationship patterns that repeatedly result in harm or isolation
- Suicidal thoughts or self-harm urges
- Inability to function at work, school, or in essential life domains due to emotional or identity difficulties
Complex trauma recovery is possible, but it typically requires professional guidance to navigate safely and effectively. Self-help strategies and peer support can complement professional treatment but generally cannot substitute for specialized trauma therapy when symptoms are severe.
Conclusion
CPTSD — affect regulation difficulties and self-concept disturbances beyond PTSD represent a distinct clinical presentation requiring specialized understanding and treatment. The emotional dysregulation in complex PTSD extends beyond trauma-specific responses to encompass pervasive challenges managing emotional states across diverse contexts. Similarly, self-concept disturbances in CPTSD involve fundamental disruptions to identity formation and self-perception that differ qualitatively from the negative cognitions seen in standard PTSD.
Recognizing these distinctive features is essential for trauma survivors seeking to understand their experiences and for clinicians developing appropriate treatment approaches. The additional symptom clusters in CPTSD—particularly around affect regulation and self-concept—require treatment strategies that prioritize stabilization, skill-building, and identity reconstruction alongside trauma processing. With appropriate support, including professional therapy and accessible resources for ongoing emotional processing, individuals with complex trauma can develop greater emotional regulation capacities and reconstruct self-concepts that integrate traumatic histories without being defined by them.
Disclaimer: This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm — seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
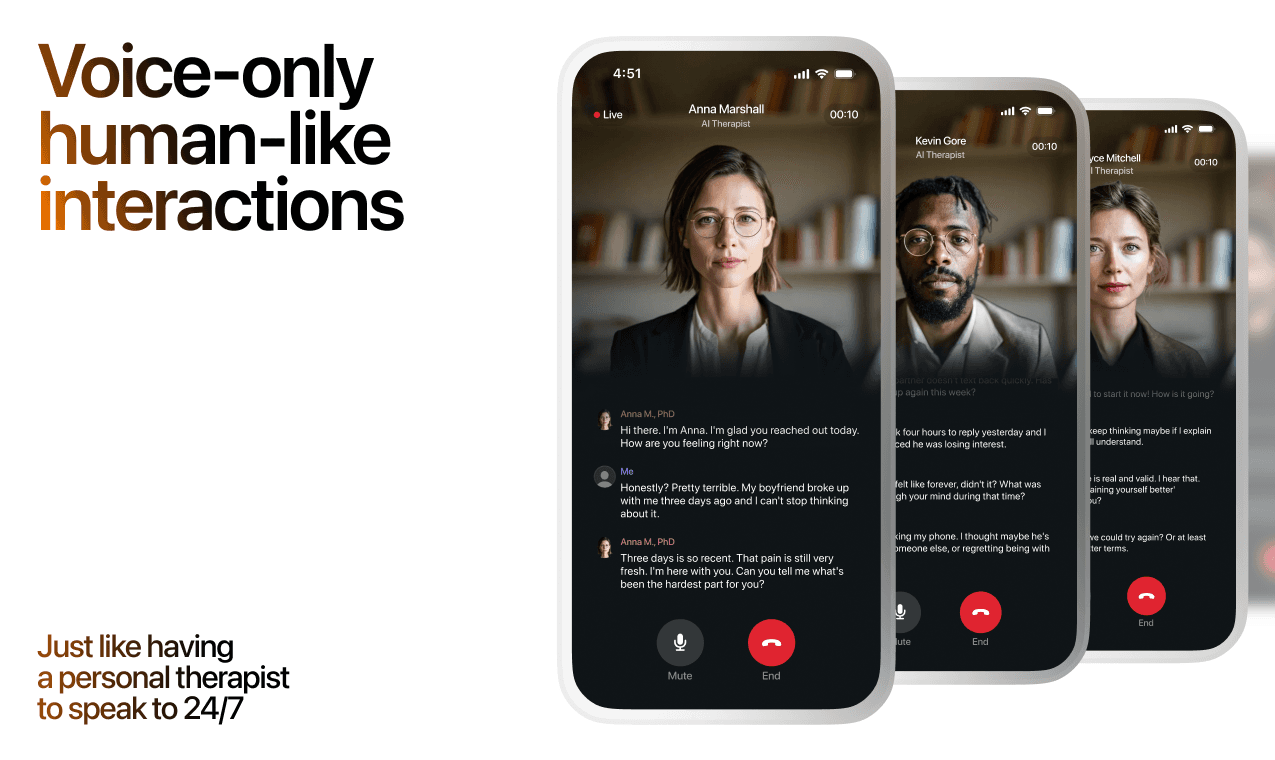
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
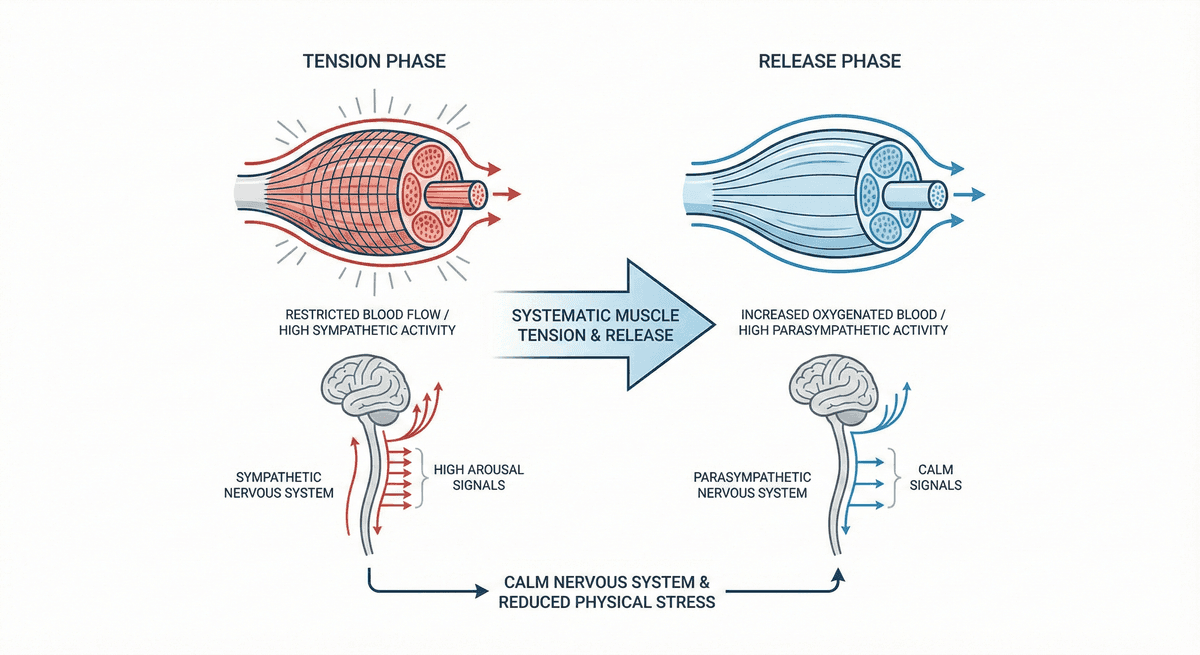
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
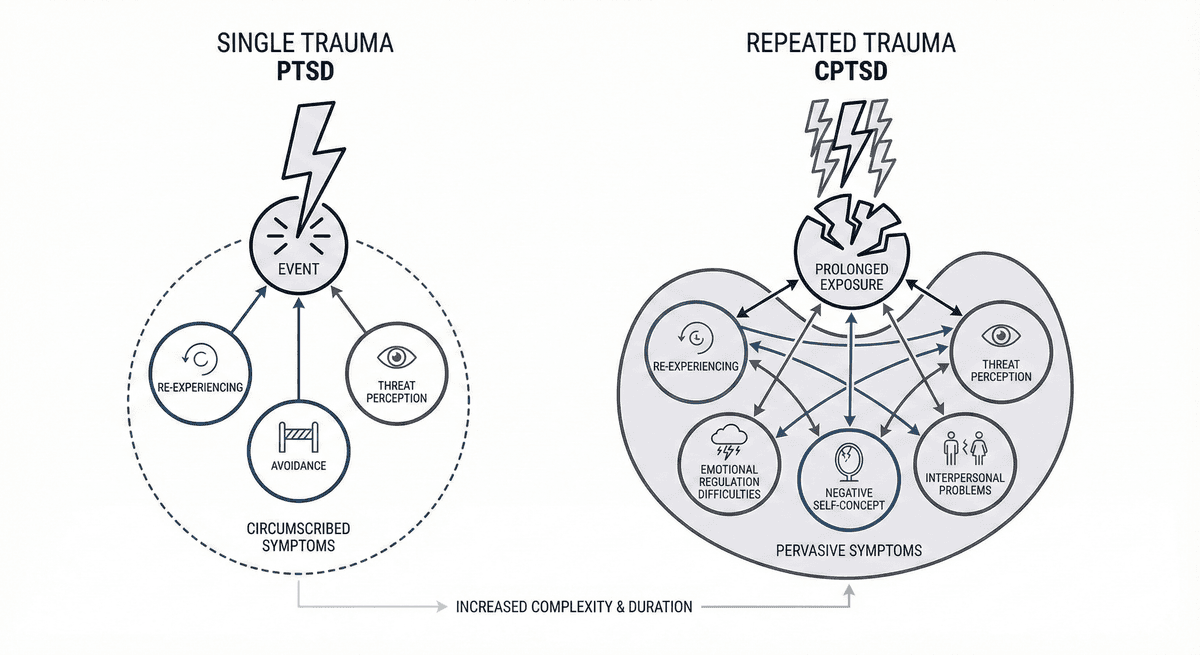
PTSD vs CPTSD: Single Trauma vs Repeated Trauma Symptom Differences
Learn how PTSD from a single traumatic event differs from CPTSD shaped by repeated trauma, including symptom patterns and treatment approaches.
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.