EMDR in Trauma Therapy — Francine Shapiro Method Integration in Clinical Practice
Eye Movement Desensitization and Reprocessing (EMDR) represents one of the most significant developments in trauma therapy since its introduction by
Key Takeaways
- History taking and treatment planning: Identifying target memories and assessing client readiness
- Preparation: Building therapeutic alliance and teaching self-regulation skills
- Assessment: Activating the memory network through specific protocols
- Desensitization: Processing traumatic material using bilateral stimulation
- Installation: Strengthening adaptive cognitions
EMDR in Trauma Therapy — Francine Shapiro Method Integration in Clinical Practice
A comprehensive guide to implementing the Francine Shapiro EMDR approach in clinical trauma treatment settings
emdr-trauma-therapy-francine-shapiro-method
Introduction
Eye Movement Desensitization and Reprocessing (EMDR) represents one of the most significant developments in trauma therapy since its introduction by psychologist Francine Shapiro. As mental health professionals increasingly seek evidence-informed approaches for treating trauma-related conditions, understanding how to integrate Francine Shapiro's EMDR method into clinical practice has become essential. This approach to EMDR in trauma therapy combines structured protocols with adaptive flexibility, allowing clinicians to address complex trauma presentations while maintaining therapeutic safety. This article explores the practical integration of Francine Shapiro's EMDR method into clinical trauma therapy practice, drawing on clinical implementation research and therapeutic best practices to provide actionable guidance for mental health professionals.
Understanding the Francine Shapiro EMDR Framework for Trauma Therapy
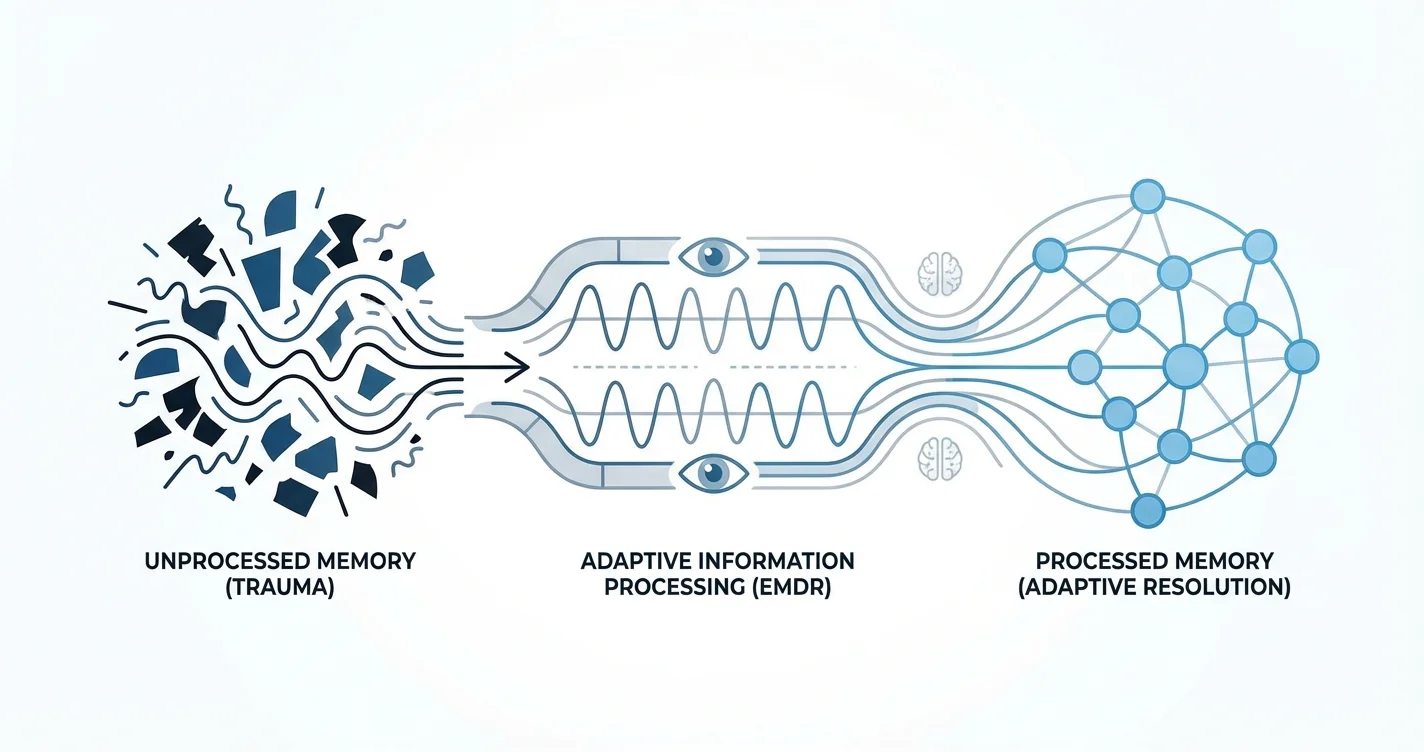
The Francine Shapiro EMDR method operates on the Adaptive Information Processing (AIP) model, which proposes that traumatic memories become maladaptively stored when overwhelming experiences exceed the brain's natural processing capacity. Research from clinical neuroscience suggests that trauma memories may remain incompletely processed, with sensory and emotional components stored separately from narrative understanding, contributing to intrusive symptoms and emotional dysregulation.
Shapiro's framework conceptualizes psychological symptoms as stemming from these unprocessed memories rather than inherent pathology. This perspective fundamentally shifts how clinicians approach trauma treatment—moving from symptom management to memory reprocessing. In clinical trauma therapy settings, this distinction influences treatment planning, case conceptualization, and the therapeutic relationship itself.
The eight-phase structure developed by Shapiro provides clinicians with a systematic approach to applying EMDR in trauma therapy:
- History taking and treatment planning: Identifying target memories and assessing client readiness
- Preparation: Building therapeutic alliance and teaching self-regulation skills
- Assessment: Activating the memory network through specific protocols
- Desensitization: Processing traumatic material using bilateral stimulation
- Installation: Strengthening adaptive cognitions
- Body scan: Identifying and processing residual somatic disturbance
- Closure: Ensuring client stability between sessions
- Reevaluation: Assessing treatment progress and identifying remaining targets
This phased approach allows for clinical flexibility while maintaining protocol integrity—a balance essential for implementing Francine Shapiro's EMDR technique in diverse clinical trauma treatment contexts.
Clinical Practice Integration of Francine Shapiro's EMDR Approach for Trauma Therapy
Integrating the Francine Shapiro EMDR method into clinical trauma therapy practice requires more than technical training—it demands thoughtful consideration of practice setting, client population, and professional competencies. Research indicates that successful EMDR implementation depends significantly on thorough preparation and proper client selection.
When establishing EMDR in trauma therapy within a clinical practice, professionals typically begin by assessing organizational readiness. This includes ensuring adequate session length (standard EMDR sessions often require 60-90 minutes), appropriate physical space for bilateral stimulation delivery, and scheduling flexibility to accommodate the intensive nature of trauma reprocessing work.
Client suitability assessment represents a critical element of integrating Francine Shapiro's EMDR method. While EMDR demonstrates broad applicability across trauma presentations, certain clinical considerations influence treatment timing and approach:
- Adequate affect regulation capacity: Clients need sufficient skills to manage emotional activation between sessions
- Stable life circumstances: Active crisis situations may require stabilization before memory reprocessing
- Readiness for trauma-focused work: Client motivation and understanding of the treatment process
- Dissociative symptom management: Complex dissociative presentations may require modified protocols
- Medical considerations: Certain conditions (recent eye surgery, pregnancy with complications, seizure disorders) warrant consultation
Clinical documentation practices also require adaptation when implementing EMDR. Treatment notes should capture the target memory, associated cognitions and emotions, subjective units of disturbance (SUD) ratings, and processing outcomes without extensively documenting traumatic content—protecting both client privacy and clinician secondary trauma exposure.
Many practitioners find that integrating accessible support tools like Lovon.app can help clients process emotional material between EMDR sessions, providing on-demand support when distressing content surfaces outside therapy hours. This type of supplemental resource can enhance treatment continuity without replacing the specialized reprocessing work of formal EMDR sessions.
Applying Francine Shapiro's EMDR Method to Trauma Therapy in Clinical Settings
The practical application of EMDR in trauma therapy using Francine Shapiro's method involves specific technical elements that distinguish it from other therapeutic approaches. Understanding these components allows clinicians to implement the treatment with fidelity while adapting to individual client needs.
Bilateral Stimulation Delivery
The signature element of Shapiro's approach involves bilateral stimulation—alternating activation of left and right hemispheres through eye movements, tactile stimulation, or auditory tones. In clinical practice settings, professionals typically begin with eye movements as the primary modality, asking clients to visually track the therapist's fingers moving horizontally across their visual field. Studies suggest that bilateral stimulation may facilitate information processing, though the precise mechanisms remain an area of ongoing investigation.
When eye movements prove difficult due to visual limitations, client discomfort, or other factors, tactile bilateral stimulation (alternating hand taps) or auditory stimulation (alternating tones through headphones) serve as effective alternatives. Experienced EMDR practitioners often develop facility with multiple modalities, adjusting based on client response and processing effectiveness.
Target Selection and Sequencing
Applying Francine Shapiro's EMDR technique in clinical trauma treatment requires strategic identification of memory targets. Rather than processing every difficult memory, clinicians work with clients to identify:
- Index trauma: The earliest or most significant trauma that established maladaptive patterns
- Current triggers: Present-day situations that activate traumatic material
- Future templates: Anticipated situations requiring adaptive response patterns
This three-pronged approach—addressing past memories, present triggers, and future scenarios—distinguishes the comprehensive nature of Shapiro's method from exposure-only approaches. Clinical experience suggests that processing the earliest related memory often creates generalization effects, with later similar experiences resolving without direct targeting.
Managing Abreactions and Processing Blocks
When implementing the Francine Shapiro EMDR method in trauma therapy clinical settings, practitioners inevitably encounter intense emotional responses (abreactions) or processing difficulties. Shapiro's protocols include specific interventions for these situations:
- Cognitive interweave: When processing stalls, the therapist introduces information that facilitates adaptive resolution
- Resource development and installation (RDI): Strengthening positive internal resources before or during trauma processing
- Containment strategies: Techniques for managing overwhelming affect during and between sessions
These interventions require clinical judgment to implement appropriately—balancing protocol fidelity with responsive adaptation to client needs. Research on EMDR implementation indicates that therapist skill in managing processing complications significantly influences treatment outcomes.
Advanced Considerations for EMDR in Trauma Therapy Implementation
As clinicians gain experience with integrating Francine Shapiro's EMDR approach into clinical trauma therapy practice, several advanced considerations emerge that extend beyond foundational training.
Complex Trauma Adaptations
While Shapiro's original protocols were validated primarily with single-incident trauma, subsequent adaptations have extended EMDR applicability to complex developmental trauma. Clients with extensive childhood trauma, attachment disruptions, or structural dissociation may require extended preparation phases, slower processing pacing, and integration of ego state or parts work before standard EMDR protocols prove effective.
Some practitioners integrate approaches like the Flash technique, progressive counting, or modified protocols specifically designed for complex presentations. However, it's important to note that these adaptations, while showing promise, may require additional specialized training beyond standard EMDR certification.
Cultural Considerations
Implementing the Francine Shapiro EMDR technique in clinical trauma treatment across diverse populations requires cultural attunement. The emphasis on direct eye contact inherent in eye movement protocols may feel uncomfortable in some cultural contexts. The concept of bilateral stimulation itself may require culturally-informed explanation. Clinicians working across cultures often find that investing additional time in preparation, relationship-building, and culturally-adapted psychoeducation enhances treatment acceptability and effectiveness.
Integration with Other Modalities
EMDR in trauma therapy using Francine Shapiro's method doesn't exist in isolation from other therapeutic approaches. Many practitioners integrate EMDR within broader treatment frameworks that include cognitive-behavioral strategies, somatic interventions, or relational psychotherapy. This integrative approach can address the multidimensional nature of trauma—targeting not only memory reprocessing but also behavioral patterns, physiological regulation, and interpersonal functioning.
Resources like Lovon.app may complement formal EMDR work by providing clients with accessible support for processing emotions and preparing for difficult therapeutic conversations, though such tools serve as supplements rather than replacements for specialized trauma therapy.
Limitations and Contraindications
Honest acknowledgment of limitations strengthens rather than undermines clinical practice. While research suggests EMDR demonstrates effectiveness across various trauma presentations, it's not universally appropriate or effective. Some clients don't respond to bilateral stimulation, find the approach too activating, or prefer alternative trauma-focused treatments. Active substance dependence, acute psychosis, unstable medical conditions, or inadequate affect regulation capacity may indicate the need for different or preliminary interventions before EMDR implementation.
Additionally, the intensive nature of EMDR work requires adequate therapist self-care practices. Regular consultation, personal therapy, and attention to vicarious traumatization help clinicians maintain the presence and attunement essential for effective trauma therapy delivery.
Conclusion
Successfully integrating Francine Shapiro's EMDR method into clinical trauma therapy practice represents both a technical and relational endeavor. Understanding the theoretical foundations of EMDR in trauma therapy—particularly the Adaptive Information Processing model—provides clinicians with a coherent framework for conceptualizing trauma symptoms and treatment mechanisms. The structured eight-phase protocol offers systematic guidance while allowing adaptive flexibility for diverse clinical presentations.
Practical implementation of the Francine Shapiro EMDR approach requires attention to organizational readiness, client selection, technical skill development, and cultural attunement. As clinicians gain experience applying Francine Shapiro's EMDR technique in clinical trauma treatment, they develop facility with bilateral stimulation modalities, target sequencing strategies, and interventions for processing complications.
For mental health professionals committed to evidence-informed trauma treatment, investing in comprehensive EMDR training, ongoing consultation, and clinical supervision provides the foundation for competent practice. While the learning curve extends beyond initial training, the capacity to offer effective trauma reprocessing significantly expands therapeutic capabilities. Whether working in private practice, community mental health, or specialized trauma treatment settings, integrating the Francine Shapiro EMDR method into clinical trauma therapy practice offers clients access to a well-researched approach for addressing the persistent effects of traumatic experiences.
When to Seek Professional Help
If you're experiencing trauma-related symptoms that interfere with daily functioning—such as intrusive memories, persistent avoidance, emotional numbness, or hypervigilance—professional support can make a significant difference. Mental health professionals trained in trauma-focused therapies, including EMDR-certified clinicians, can provide specialized assessment and treatment. If symptoms are worsening, if you're experiencing thoughts of self-harm, or if trauma reactions are significantly affecting relationships or work, reaching out to a trauma-informed therapist, psychologist, or psychiatrist is an important step. EMDR therapy is typically delivered by licensed mental health professionals who have completed specialized training in the Francine Shapiro method.
Disclaimer
This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm—seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
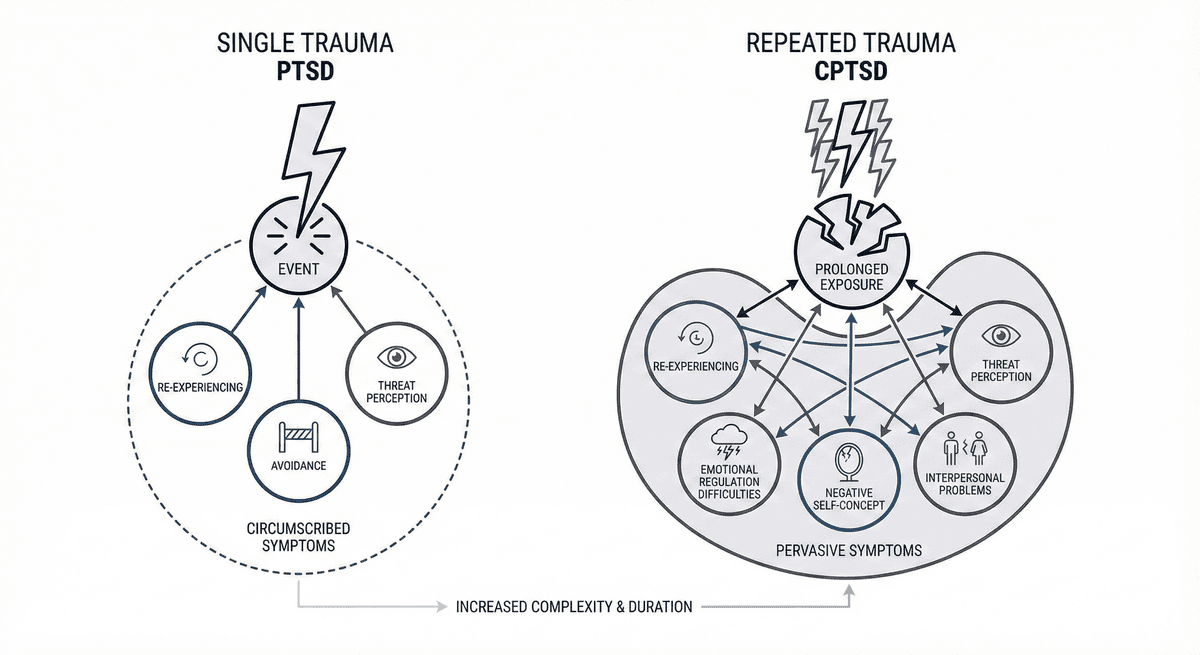
PTSD vs CPTSD: Single Trauma vs Repeated Trauma Symptom Differences
Learn how PTSD from a single traumatic event differs from CPTSD shaped by repeated trauma, including symptom patterns and treatment approaches.
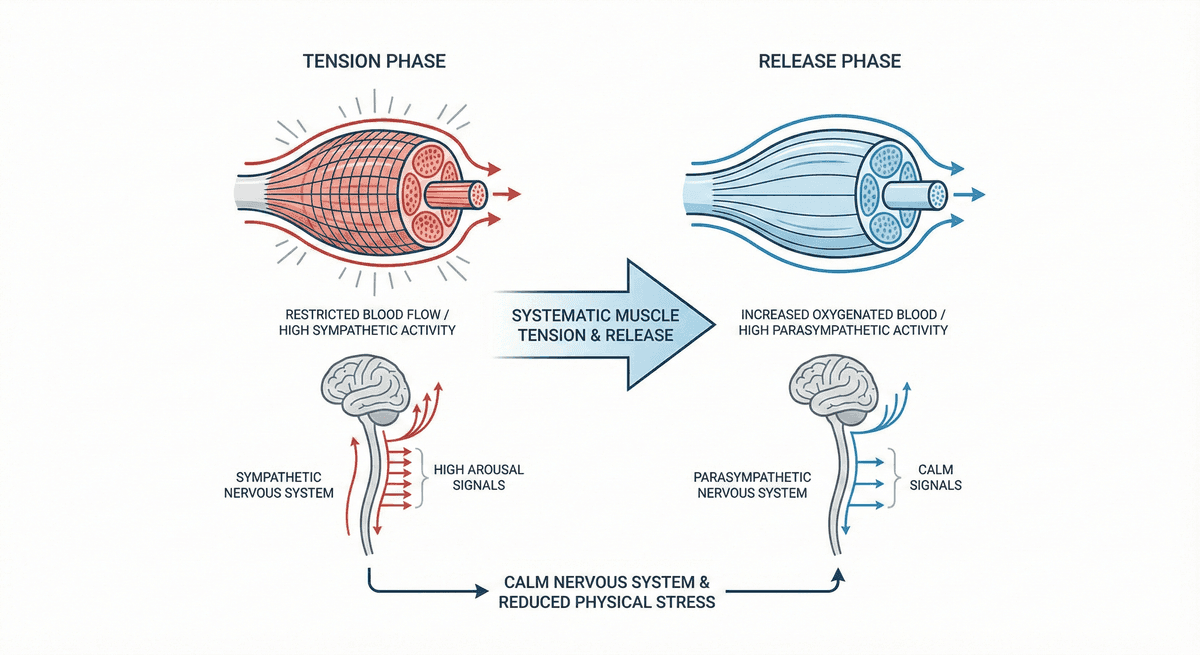
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.