Bipolar 1 vs Bipolar 2 vs Cyclothymia: Key Differences Explained
Navigating the landscape of mood disorders can feel overwhelming, especially when trying to understand the differences between Bipolar 1 vs Bipolar 2 vs...
Key Takeaways
- Significantly decreased need for sleep (feeling rested after only a few hours)
- Rapid, pressured speech that's difficult to interrupt
- Racing thoughts or flight of ideas
- Increased goal-directed activity or psychomotor agitation
- Inflated self-esteem or grandiosity
Introduction
Navigating the landscape of mood disorders can feel overwhelming, especially when trying to understand the differences between Bipolar 1 vs Bipolar 2 vs Cyclothymia. These three conditions share a common thread—cyclical mood fluctuations—but differ significantly in their severity, duration, and impact on daily functioning. According to mental health professionals, cyclothymic disorder is particularly overlooked despite being a distinct cyclical mood disorder alongside bipolar conditions. This article provides an evidence-based exploration of how these three conditions differ, helping you recognize their unique characteristics and understand when professional evaluation becomes essential. The information presented draws from clinical expertise and current diagnostic frameworks used by mental health practitioners.
Understanding Cyclical Mood Disorders
The Diagnostic and Statistical Manual of Mental Disorders (DSM) recognizes multiple mood disorders characterized by fluctuating emotional states. While Major Depressive Disorder represents one end of the mood disorder spectrum with substantial unpredictable ups and downs, bipolar conditions and cyclothymia involve distinct patterns of both elevated and depressed moods.
Cyclical mood disorders differ fundamentally from chronic, stable conditions like Persistent Depressive Disorder, which involves fairly constant sadness with minimal fluctuations. Instead, these conditions feature unpredictable mood changes that cycle over time, creating challenges in daily functioning and relationships.
Mental health practitioners note that many professionals remain unaware of cyclothymia as a distinct diagnostic category, despite it being the third major cyclical mood disorder. This lack of awareness can lead to misdiagnosis or delayed treatment for individuals experiencing chronic emotional highs and lows that don't meet criteria for full bipolar disorder.
Bipolar 1 Disorder: Defining Characteristics
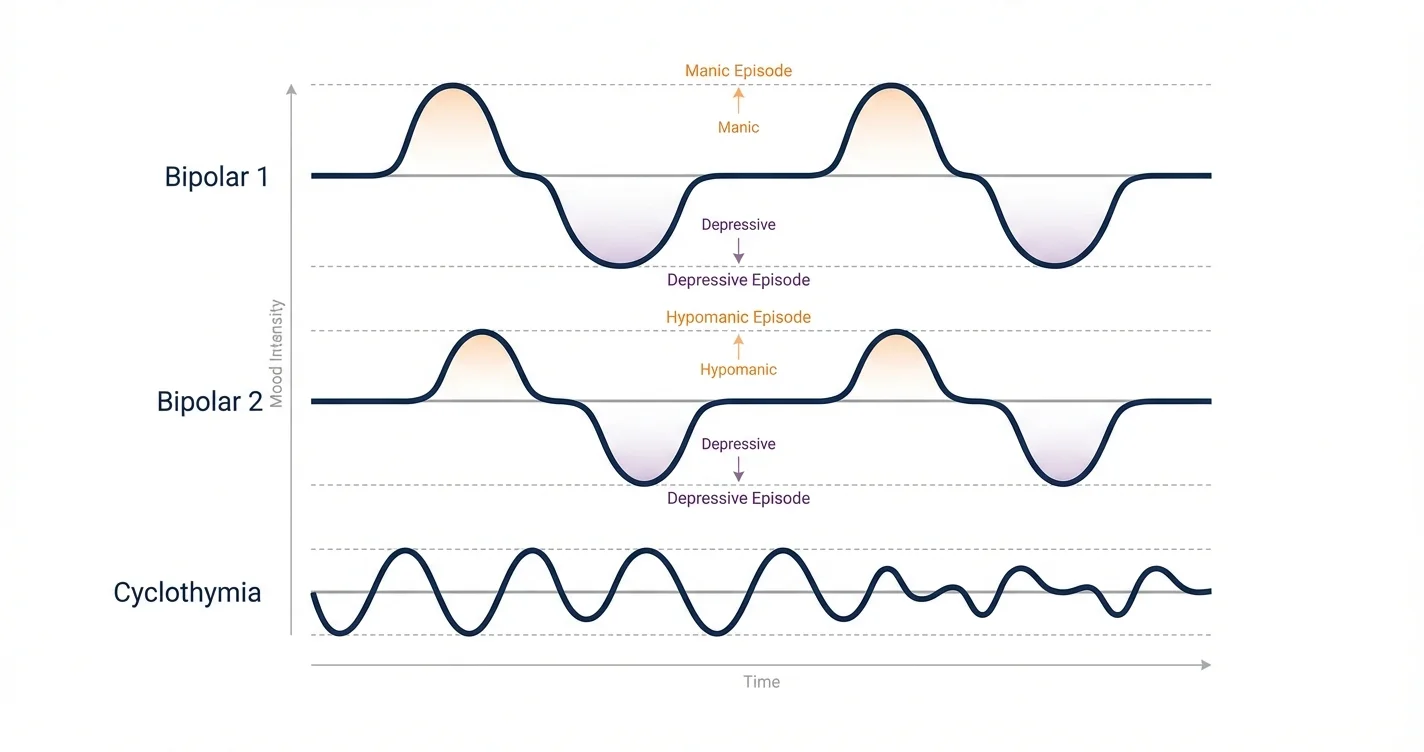
Bipolar 1 disorder represents the most severe form of bipolar spectrum conditions, characterized by the occurrence of at least one manic episode. These manic episodes involve distinct periods of abnormally elevated, expansive, or irritable mood lasting at least one week (or requiring hospitalization).
Core Features of Manic Episodes
During manic episodes, individuals may experience:
- Significantly decreased need for sleep (feeling rested after only a few hours)
- Rapid, pressured speech that's difficult to interrupt
- Racing thoughts or flight of ideas
- Increased goal-directed activity or psychomotor agitation
- Inflated self-esteem or grandiosity
- Excessive involvement in activities with potentially painful consequences
- Marked impairment in social or occupational functioning
Research indicates that manic episodes often require hospitalization due to safety concerns or severe functional impairment. The intensity distinguishes these episodes from less severe hypomanic states seen in other conditions.
Individuals with Bipolar 1 typically also experience depressive episodes, though these aren't required for diagnosis. The depressive phases can be equally debilitating, involving profound sadness, loss of interest in activities, changes in sleep and appetite, and sometimes thoughts of self-harm.
Bipolar 2 Disorder: Hypomania and Depression
Bipolar 2 disorder differs fundamentally from Bipolar 1 in that it never involves full manic episodes. Instead, individuals experience hypomanic episodes—elevated mood states that are noticeable but don't cause the severe impairment characteristic of mania.
Understanding Hypomania
Hypomanic episodes share many features with mania but are:
- Shorter in minimum duration (at least four consecutive days)
- Less severe in intensity
- Not associated with psychotic features
- Not causing marked impairment in functioning
- Sometimes experienced as productive or even pleasant periods
Clinical experience suggests that hypomania can be challenging to identify because individuals may feel unusually creative, energetic, or productive during these periods. Family members or close friends often notice the changes more readily than the person experiencing them.
The Depressive Component
For a Bipolar 2 diagnosis, individuals must experience at least one major depressive episode. These depressive periods often cause more distress and functional impairment than the hypomanic episodes. Studies indicate that people with Bipolar 2 spend considerably more time in depressive states than in elevated moods, which significantly impacts quality of life and sometimes leads to initial misdiagnosis as unipolar depression.
The depressive episodes in Bipolar 2 are clinically indistinguishable from those in Major Depressive Disorder or Bipolar 1, involving the same symptoms of low mood, anhedonia, sleep disturbances, and concentration difficulties.
Cyclothymia: Chronic Mood Instability
Cyclothymic disorder represents a milder but chronic pattern of mood fluctuations. Mental health experts emphasize that cyclothymia is commonly overlooked despite causing significant emotional distress and functional challenges.
Diagnostic Criteria and Patterns
Cyclothymia involves:
- Numerous periods of hypomanic symptoms (not meeting full criteria for hypomania)
- Numerous periods of depressive symptoms (not meeting full criteria for major depression)
- Duration of at least two years in adults (one year in children/adolescents)
- Symptoms present for more than half the time
- No symptom-free periods longer than two months
The chronic nature distinguishes cyclothymia from episodic bipolar conditions. Rather than distinct episodes with clear beginnings and endings, individuals experience relatively continuous mood fluctuations without full remission.
Clinical Presentation
People with cyclothymia describe their experience as riding an emotional rollercoaster without the extreme highs or devastating lows of bipolar disorder. The fluctuations, while less intense, create persistent challenges in:
- Maintaining consistent work performance
- Sustaining stable relationships
- Planning for the future with unpredictable mood states
- Managing energy levels and motivation
Research suggests that cyclothymia may represent a risk factor for later development of bipolar disorder, with some individuals eventually experiencing episodes that meet full diagnostic criteria. However, many people maintain a cyclothymic pattern throughout their lives without progression to bipolar disorder.
Comparing Severity and Functional Impact
When examining Bipolar 1 vs Bipolar 2 vs Cyclothymia, severity exists on a spectrum. Bipolar 1 typically causes the most severe disruption, with manic episodes often requiring hospitalization and creating significant safety concerns. The elevated mood states can lead to impulsive decisions with lasting consequences—financial devastation, damaged relationships, or legal problems.
Bipolar 2, while lacking full mania, often involves profound suffering during depressive episodes. Some research indicates that Bipolar 2 may carry higher suicide risk than Bipolar 1, possibly because depressive episodes predominate and hypomanic periods may go unrecognized, delaying appropriate treatment.
Cyclothymia, though milder in episode severity, creates cumulative impairment through chronicity. The persistent mood instability affects long-term planning, career advancement, and relationship stability. Individuals may struggle to explain their inconsistent functioning to employers, partners, or family members.
Treatment Approaches and Considerations
Treatment strategies differ somewhat across these three conditions, though they share common elements. Mood stabilizers form the foundation of bipolar disorder treatment, while cyclothymia may respond to psychotherapy alone or in combination with medication.
Professional Evaluation Is Essential
Distinguishing between these conditions requires comprehensive psychiatric evaluation. Mental health practitioners consider:
- Detailed symptom history and timeline
- Family history of mood disorders
- Impact on functioning across different life domains
- Response to previous treatments (if any)
- Substance use patterns that may complicate the picture
Self-diagnosis is particularly problematic with mood disorders because individuals often lack clear perspective on their symptoms during mood episodes. What feels like normal happiness might represent hypomania, while persistent low mood might be dismissed as "just stress."
Ongoing Support Strategies
Between professional appointments, individuals can benefit from structured support. Tools like Lovon.app provide accessible resources for processing emotions and recognizing patterns as they emerge. This on-demand support can help people prepare for conversations with their treatment providers and develop greater awareness of their mood fluctuations.
Psychotherapy, particularly cognitive-behavioral approaches and interpersonal therapy, helps individuals develop coping strategies, recognize early warning signs of mood episodes, and maintain treatment adherence. For many people with cyclothymia, psychotherapy represents the primary treatment approach.
When to Seek Professional Help
Understanding the differences between Bipolar 1 vs Bipolar 2 vs Cyclothymia is valuable, but recognizing when professional evaluation becomes necessary is critical. Seek assessment from a mental health professional if you experience:
- Periods of unusually elevated mood, increased energy, or decreased need for sleep
- Distinct episodes of depression lasting two weeks or longer
- Chronic mood fluctuations that affect your relationships or work performance
- Impulsive behaviors during high-energy periods that you later regret
- Thoughts of self-harm or suicide during low periods
- Family history of bipolar disorder combined with mood instability
Mental health professionals who can provide comprehensive evaluation include psychiatrists, psychiatric nurse practitioners, and licensed psychologists with experience in mood disorders. Some may specialize specifically in bipolar spectrum conditions.
For individuals already in treatment, tools like Lovon.app can complement professional care by providing support for processing difficult emotions between sessions and working through relationship conflicts that often arise with mood instability. However, these resources work best as part of a comprehensive treatment plan rather than as standalone interventions.
If you're experiencing a mental health crisis, immediate professional help is essential. Mental health treatment is most effective when it addresses your specific diagnosis and symptom pattern, which is why accurate evaluation matters so profoundly.
Conclusion
Distinguishing between Bipolar 1 vs Bipolar 2 vs Cyclothymia requires understanding the intensity, duration, and pattern of mood fluctuations characteristic of each condition. Bipolar 1 involves severe manic episodes; Bipolar 2 features hypomania with significant depressive episodes; and cyclothymia presents as chronic, milder fluctuations without full episodes. Each condition creates distinct challenges and responds to different treatment approaches, making accurate diagnosis essential for effective care. If you recognize patterns of mood instability in your own experience, comprehensive evaluation by a qualified mental health professional provides the foundation for appropriate treatment and improved quality of life. Understanding these differences empowers you to seek the right support and engage more effectively with your treatment team.
Disclaimer: This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm — seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
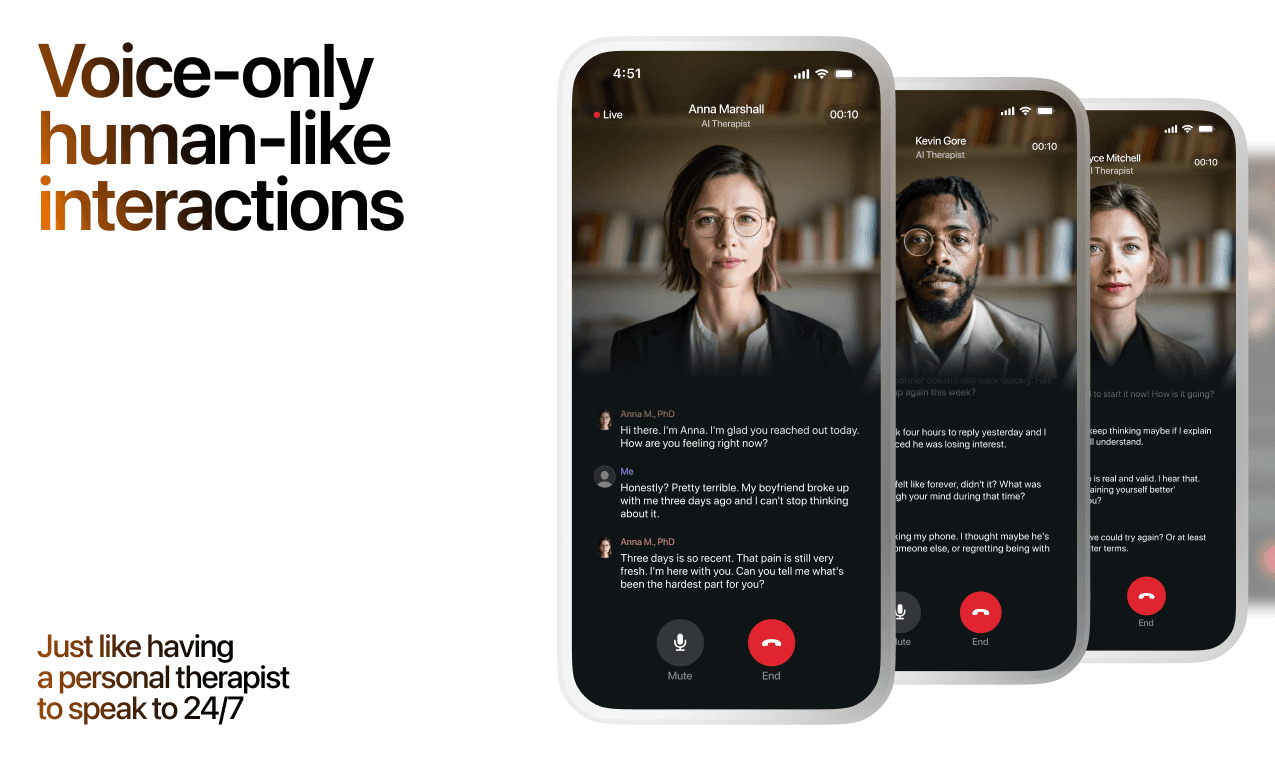
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
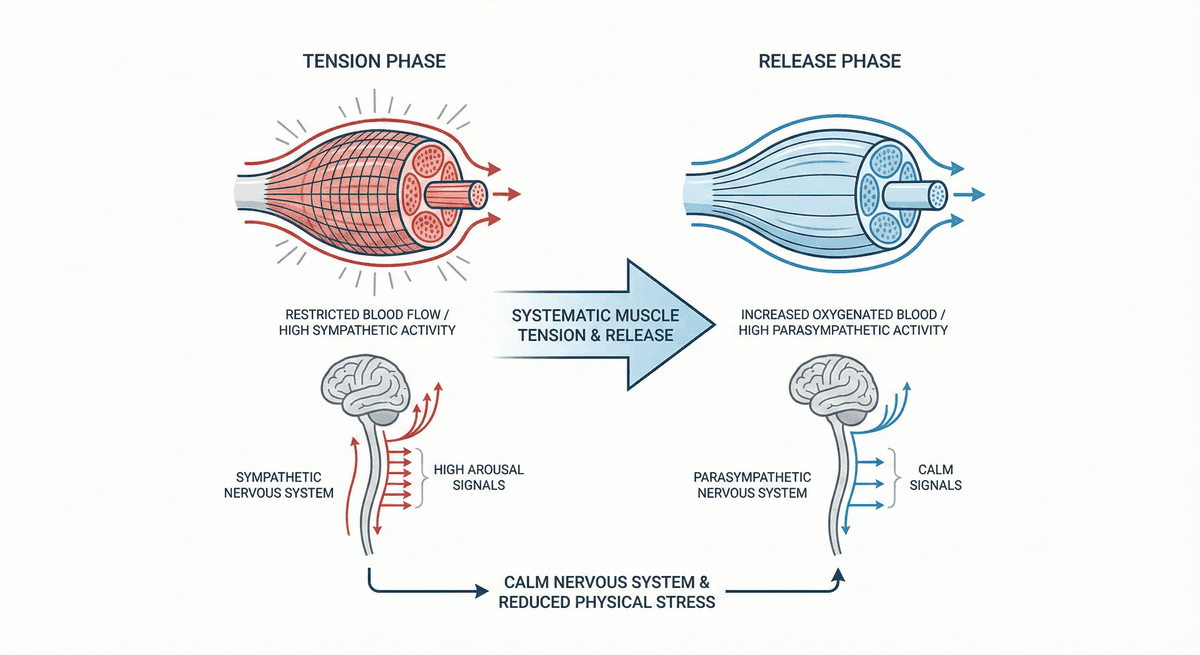
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.