Disorganized Attachment Style: Causes & Recovery 2026
Disorganized attachment style causes constant push-pull in relationships. Learn what drives it, 6 evidence-based recovery steps, and on-demand support tools for 2026.
Key Takeaways
- A trauma-informed therapist — EMDR, somatic therapy, or IFS-trained clinicians have the strongest evidence base for
- A regulation tool for between sessions — an app, a journaling practice, or a breathwork protocol you can reach in
- One safe relationship — it does not have to be romantic. A consistent, low-stakes connection with a friend, sibling,
- Basic knowledge of your window of tolerance — knowing when you are hyperactivated (anxiety, rage, clinging) versus
- 30–60 minutes per day — not for formal therapy, but for the micro-practices in the steps below.
Disorganized attachment style is the least understood and most disruptive of the four attachment patterns — and if you have it, everyday relationships can feel like emotional minefields you can never fully map.
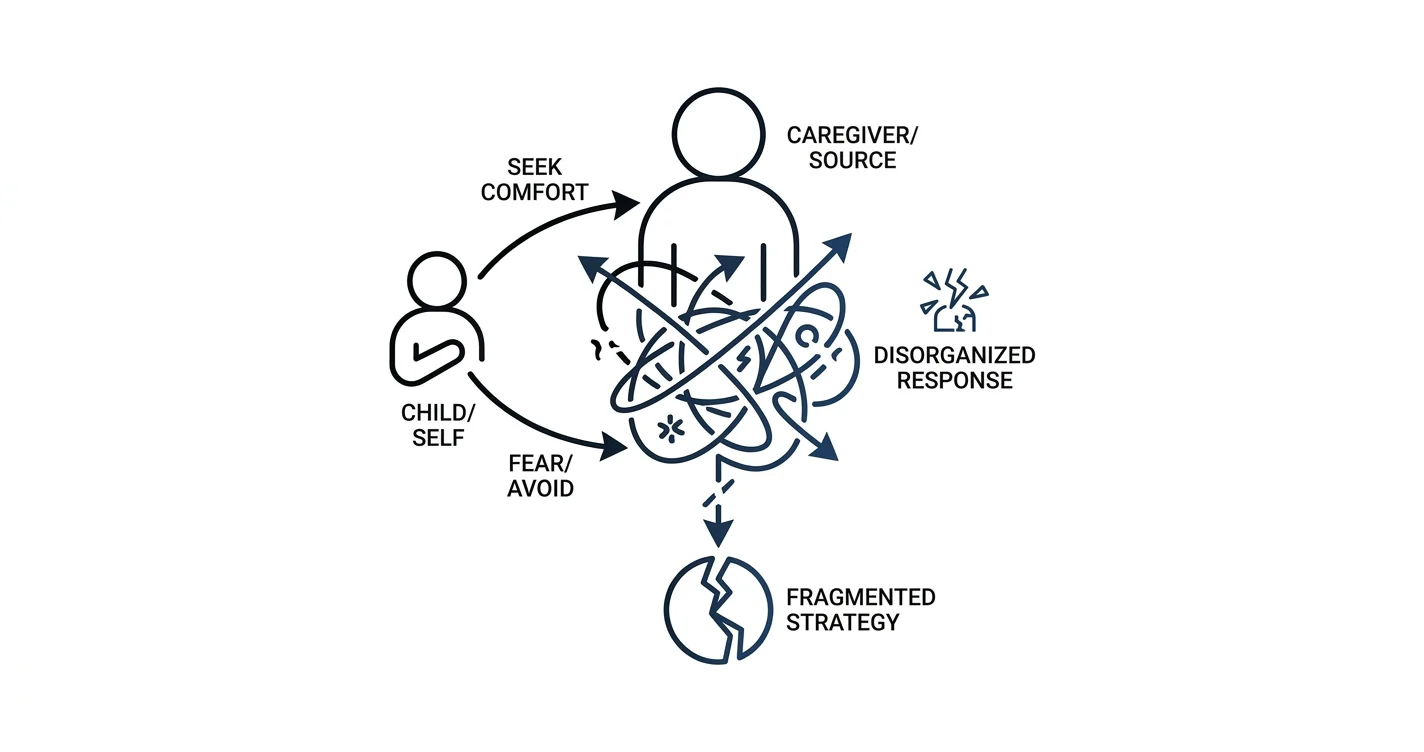
TL;DR: Disorganized attachment style develops when a primary caregiver was both a source of comfort and a source of fear during childhood. Adults with this pattern oscillate between craving closeness and fleeing from it, often without knowing why. Recovery is real in 2026 — it requires trauma-informed therapy, nervous system regulation, and consistent relational practice. Lovon's AI voice therapy app offers on-demand support between formal sessions for people working through disorganized attachment.
Why this matters
Attachment research, beginning with Mary Ainsworth's Strange Situation studies in the 1970s and extended by Mary Main's work in the 1980s, identified disorganized attachment as the pattern most strongly linked to later trauma responses, dissociation, and relational instability. A 2019 meta-analysis in Psychological Bulletin found that disorganized attachment in infancy predicted significantly elevated rates of psychopathology in adulthood compared to all other insecure styles. This is not a personality flaw — it is a learned survival strategy that outlived its usefulness.
What you'll need
Before working through the steps below, put these in place:
- A trauma-informed therapist — EMDR, somatic therapy, or IFS-trained clinicians have the strongest evidence base for disorganized attachment. Expect a minimum commitment of 6–12 months of weekly sessions.
- A regulation tool for between sessions — an app, a journaling practice, or a breathwork protocol you can reach in under 60 seconds.
- One safe relationship — it does not have to be romantic. A consistent, low-stakes connection with a friend, sibling, or peer support group is enough to practice with.
- Basic knowledge of your window of tolerance — knowing when you are hyperactivated (anxiety, rage, clinging) versus hypoactivated (shutdown, dissociation, numbness) is foundational.
- 30–60 minutes per day — not for formal therapy, but for the micro-practices in the steps below.
The steps
Step 1: Name the pattern accurately
What it accomplishes: You cannot change a behavior you keep misidentifying. Many people with disorganized attachment spend years treating themselves as "just anxious" or "just avoidant," which misses the disorganized driver entirely.
Why it matters: Disorganized attachment is not a midpoint between anxious and avoidant. It is its own category, rooted in what attachment researchers call "fright without solution" — the experience of needing your caregiver while simultaneously fearing them. The result is a collapse of coherent strategy.
Specific signs to recognize in yourself:
- You pursue closeness intensely, then feel suffocated when you get it — sometimes within hours.
- Conflict triggers freeze responses: you go blank, dissociate, or "lose time."
- You have fragmented or contradictory memories of childhood caregivers (idealized one moment, dreaded the next).
- You fear both abandonment and engulfment, sometimes simultaneously.
Expected outcome: Labeling the pattern correctly reframes self-blame as neurobiological history. That shift reduces shame enough to make the next steps possible.
Common mistake: Accepting an anxious-attachment label because it sounds less severe. If the freeze response and the contradictory pull-push dynamic are present, disorganized is the more accurate frame.
Step 2: Map your nervous system states
What it accomplishes: Disorganized attachment produces unpredictable nervous system swings. Polyvagal theory (Stephen Porges, 1994 and refined through 2026) describes three primary states: ventral vagal (safe, connected), sympathetic (fight/flight), and dorsal vagal (shutdown/freeze). Disorganized attaches tend to cycle through all three within a single interaction.
Why it matters: Recovery requires knowing which state you are in while you are in it, not 24 hours later in retrospect.
Instructions:
- For 7 consecutive days, log 3 check-ins per day (morning, afternoon, evening) — just 2 sentences: what state you are in and what triggered the shift.
- After 7 days, look for the triggers that reliably move you into freeze or fight/flight.
- Build a "state menu" — a short list of what brings you back to regulated from each dysregulated state. Cold water on the face, a 4-7-8 breath, a body scan, a specific song.
Expected outcome: Within 2–3 weeks most people identify 3–5 reliable triggers and 2–3 reliable regulators. That is enough to interrupt the cycle before it escalates.
Common mistake: Journaling about content (what was said) rather than state (what happened in your body). Content analysis is useful later; state mapping comes first.
Step 3: Process the origin trauma
What it accomplishes: Disorganized attachment is almost always anchored to specific relational trauma — abuse, neglect, loss of a caregiver, or living with a caregiver who was themselves traumatized and frightening. The nervous system patterns cannot fully shift until those memories are processed, not just understood intellectually.
Why it matters: Insight alone does not rewire attachment. A 2020 study in Journal of Traumatic Stress found that EMDR produced measurable changes in attachment security ratings after 12 sessions in adults with complex trauma histories. Somatic Experiencing and IFS showed comparable findings in smaller studies through 2026.
Instructions:
- Work with a trained clinician. This step is not a solo project.
- Between sessions, use stabilization-first techniques: grounding (name 5 things you see), containment imagery, and titrated exposure (approaching the memory only as far as you can stay regulated).
- Do not push for "processing" before stabilization is established — this is the single most common therapy error with disorganized clients.
Expected outcome: Reduced emotional charge when accessing difficult memories. The memory stays factual but stops triggering a full body threat response.
Common mistake: Trying to process trauma without a regulated window first. Flooding (re-traumatizing yourself by pushing too hard) reinforces the pattern rather than changing it.
Step 4: Build earned security through relational practice
What it accomplishes: Attachment styles are not fixed in childhood. "Earned secure attachment" is a documented phenomenon — adults who develop consistent, responsive relationships later in life show neural and behavioral changes consistent with secure attachment, even when their childhood pattern was disorganized.
Why it matters: The vehicle for change is repeated relational experience, not just internal work. You need to practice tolerating closeness without fleeing and tolerating distance without catastrophizing — in real time, with a real person.
Instructions:
- Choose one relationship to practice in. Make it low-stakes at first (a friend, a therapist, a peer support group).
- Set a weekly "relationship experiment" — one interaction where you deliberately do the opposite of your default. If you default to withdrawal, reach out. If you default to clinging, allow space.
- Debrief the experiment: what state did it trigger? Did you survive it? What was the actual outcome vs. the feared outcome?
- Track the gap between feared outcomes and actual outcomes over 3 months. This gap is the evidence your nervous system needs.
Expected outcome: Gradual reduction in the intensity of threat responses during closeness. Most people report meaningful change in relational tolerance within 6–9 months of consistent practice.
Common mistake: Expecting a romantic relationship to do all this work. Romantic attachment activates the deepest threat responses. Start with lower-stakes relationships and build up.
Step 5: Use on-demand support to bridge between sessions
What it accomplishes: Weekly therapy leaves 167 hours between sessions. Disorganized attachment crises rarely schedule themselves for Tuesday at 3 PM. On-demand support fills the gap.
Why it matters: Research on trauma treatment consistently shows that between-session skill use is one of the strongest predictors of outcome. What you do in the other 167 hours matters as much as the 50-minute session.
Instructions:
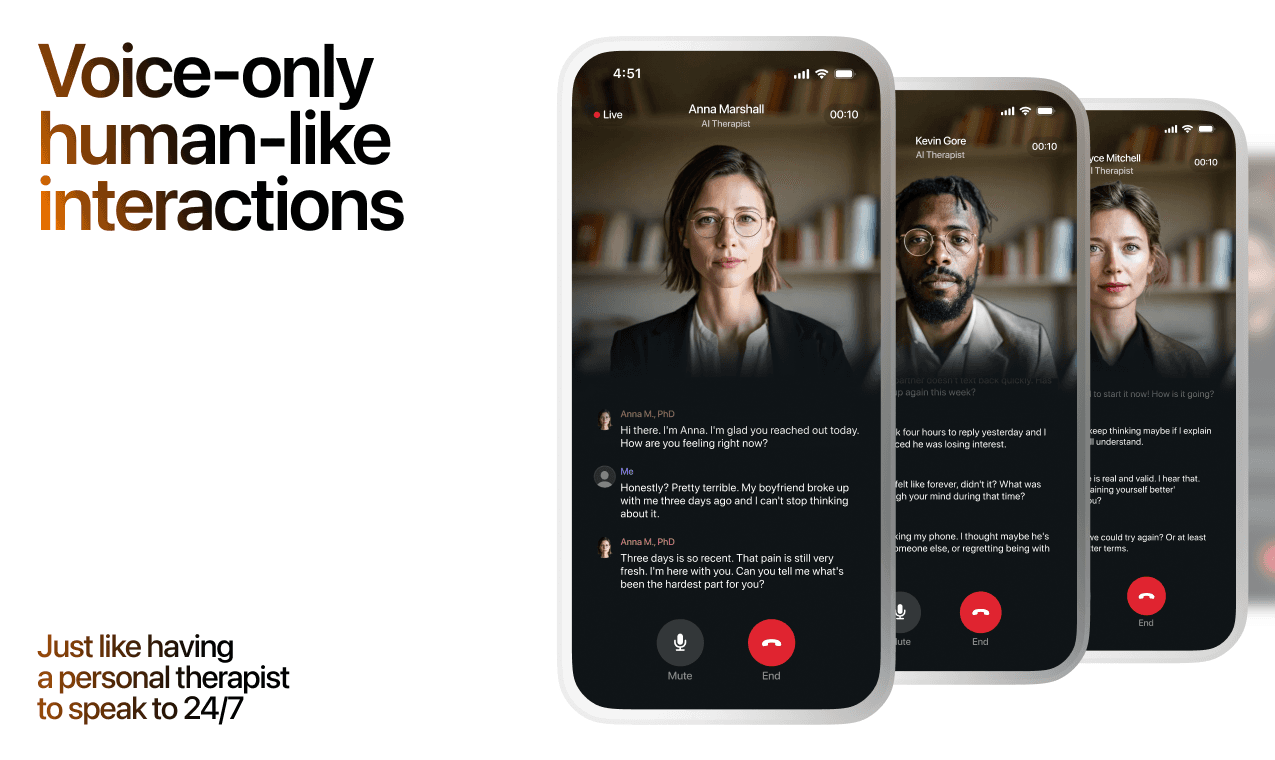
- Identify an app or resource you can access within 2 minutes of feeling dysregulated. Lovon's AI voice therapy app is built for exactly this — on-demand emotional support, coping tools, and personalized sessions available any time, specifically for anxiety, relationship stress, and trauma-adjacent emotional states.
- Use it before full dysregulation hits, not after. Catch yourself at a 5/10 distress level, not a 9/10.
- Log what worked and bring those notes to your next formal therapy session.
Expected outcome: Faster return to baseline after triggers. Over time, the window of tolerance widens because you are catching dysregulation earlier.
Common mistake: Waiting until you are fully flooded before reaching for a tool. At 9/10 distress, almost no coping tool works. The tool is for the 4/10 warning signs.
Step 6: Measure progress accurately
What it accomplishes: Recovery from disorganized attachment is nonlinear and easy to underestimate. Without measurement, people often quit right before a real threshold shift.
Why it matters: Attachment change does not feel dramatic in the moment. It shows up as a slightly shorter recovery time after conflict, a slightly lower spike in the threat response — not a cinematic epiphany.
Instructions:
- Every 30 days, rate yourself on 3 items on a 1–10 scale: (1) How quickly do I return to baseline after relational conflict? (2) How often do I pursue closeness without immediately regretting it? (3) How clearly can I identify what I need in a relationship and ask for it?
- Track those 3 numbers across 2026. A 1–2 point improvement across 6 months is clinically meaningful progress.
Expected outcome: A visible upward trend across 9–12 months that gives your nervous system evidence the work is changing something real.
Common mistake: Using mood as the only metric. Mood fluctuates for dozens of reasons. Attachment-specific behavioral markers are more accurate.
Troubleshooting
"I start therapy and then self-sabotage or quit." This is an extremely common disorganized attachment behavior — the therapeutic relationship itself activates the attachment system, which triggers fear. Name this pattern explicitly with your therapist before it happens. Agree in advance on a protocol: if you want to quit, you will attend one more session to discuss it before deciding.
"I feel worse in the first few months of working on this." Stabilization work often increases emotional awareness before it decreases distress. The emotions were already there — now you are noticing them. This is progress, not regression. It typically levels out between months 3–6.
"My partner has a different attachment style and we keep triggering each other." Disorganized plus anxious or avoidant pairings are particularly high-activation. Consider an attachment style compatibility quiz for partners to make both dynamics visible before working on the relational piece together.
"I dissociate and lose hours — I can't track my states." Dissociation above a threshold level requires clinical support before self-directed tracking. This is a sign to prioritize finding a trauma-specialized clinician rather than doing more solo work.
"I've read everything about attachment theory but nothing changes." Intellectual understanding is almost never sufficient for disorganized attachment. The change mechanism is experiential and somatic, not conceptual. This is the most common reason smart, well-informed people stay stuck — they have replaced the relational practice with more reading.
"I don't trust apps or AI tools for something this serious." Legitimate concern. AI tools are not replacements for trauma-informed human therapy in disorganized attachment cases. They are between-session regulation support only. If you are in active crisis, contact a licensed professional or a crisis line (988 in the US, active 2026).
Tools and resources
- Trauma-informed therapy directory: Psychology Today's therapist finder, filtered by EMDR or somatic therapy, is the fastest way to find a qualified clinician in your area.
- Books with strong evidence bases: Attached by Amir Levine and Rachel Heller (accessible entry point); The Body Keeps the Score by Bessel van der Kolk (trauma mechanisms); Healing the Fragmented Selves of Trauma Survivors by Janina Fisher (specifically addresses disorganized patterns).
- On-demand emotional support: Lovon's AI voice therapy app — available for anxiety, relationship stress, and emotional regulation between sessions. Relevant for anyone managing the daily volatility of disorganized attachment in 2026.
- Peer support: Attachment-focused support communities on Reddit (r/attachment_theory) and in-person NAMI groups offer low-stakes relational practice environments.
- AI relationship coaching for trust issues: If the relational piece is the current sticking point, AI relationship coach for trust issues addresses the specific dynamics that surface in disorganized patterns.
What to do next
If disorganized attachment is active in a current relationship, the next layer of work is understanding how your pattern interacts with your partner's. The AI therapy for PTSD and trauma recovery guide covers the overlap between complex trauma histories and attachment disruption — which is the terrain most disorganized attaches are actually navigating in 2026.
FAQ
What causes disorganized attachment style? Disorganized attachment forms when the primary caregiver in early childhood is simultaneously the source of comfort and the source of fear — through abuse, severe neglect, or a caregiver who was themselves traumatized and unpredictable. The child cannot develop a coherent strategy for managing distress.
Can you recover from disorganized attachment style? Yes. "Earned secure attachment" is a documented outcome in adults who received consistent trauma-informed therapy and built stable relationships later in life. Most research suggests 12–24 months of sustained work produces measurable change.
How is disorganized attachment different from anxious attachment? Anxious attachment produces a consistent strategy: pursue closeness, amplify distress signals, seek reassurance. Disorganized attachment produces no consistent strategy — the person simultaneously wants closeness and fears it, often within a single interaction. Freeze responses and dissociation are much more common in disorganized than anxious.
What does disorganized attachment look like in adult relationships? Intense idealization of a new partner followed by sudden devaluation. Pushing a partner away after achieving closeness. Freezing during conflict. Fragmented narratives about past relationships. Fear of both abandonment and intimacy coexisting.
Is disorganized attachment the same as borderline personality disorder? No. Disorganized attachment is a relational pattern with developmental roots; BPD is a clinical diagnosis defined by specific diagnostic criteria. They overlap significantly — disorganized attachment is considered a major risk factor for BPD — but many people with disorganized attachment do not meet BPD criteria, and not all BPD diagnoses involve disorganized attachment.
How long does it take to change a disorganized attachment style? Based on aggregated clinical data, most people see meaningful behavioral change in 12–18 months of consistent trauma-focused therapy. Neural and physiological markers of change take longer. There is no six-week fix for a pattern built over the first years of life.
What kind of therapy works best for disorganized attachment? EMDR, Somatic Experiencing, and Internal Family Systems (IFS) have the strongest evidence bases for disorganized attachment specifically. Standard CBT-only approaches show weaker outcomes because disorganized attachment is a somatic and relational problem, not primarily a thought-pattern problem.
Can an AI app actually help with disorganized attachment? Not as a replacement for human therapy in serious cases. AI tools are most useful for between-session regulation support — catching dysregulation early, running through coping protocols, and tracking patterns over time. Lovon is designed for exactly that role in 2026: accessible on-demand emotional support that works alongside, not instead of, clinical care.
One last thing
Mary Main's Adult Attachment Interview — the 20-question research tool used to classify adult attachment — does not score what happened to you. It scores how coherently you can talk about it. Adults classified as securely attached often had difficult childhoods. What separated them was narrative coherence: the ability to give a clear, consistent, non-contradictory account of their experience. That coherence is learnable. It is, in fact, what good trauma therapy is largely building. The destination is not a perfect childhood — it is a coherent story about the one you actually had.
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
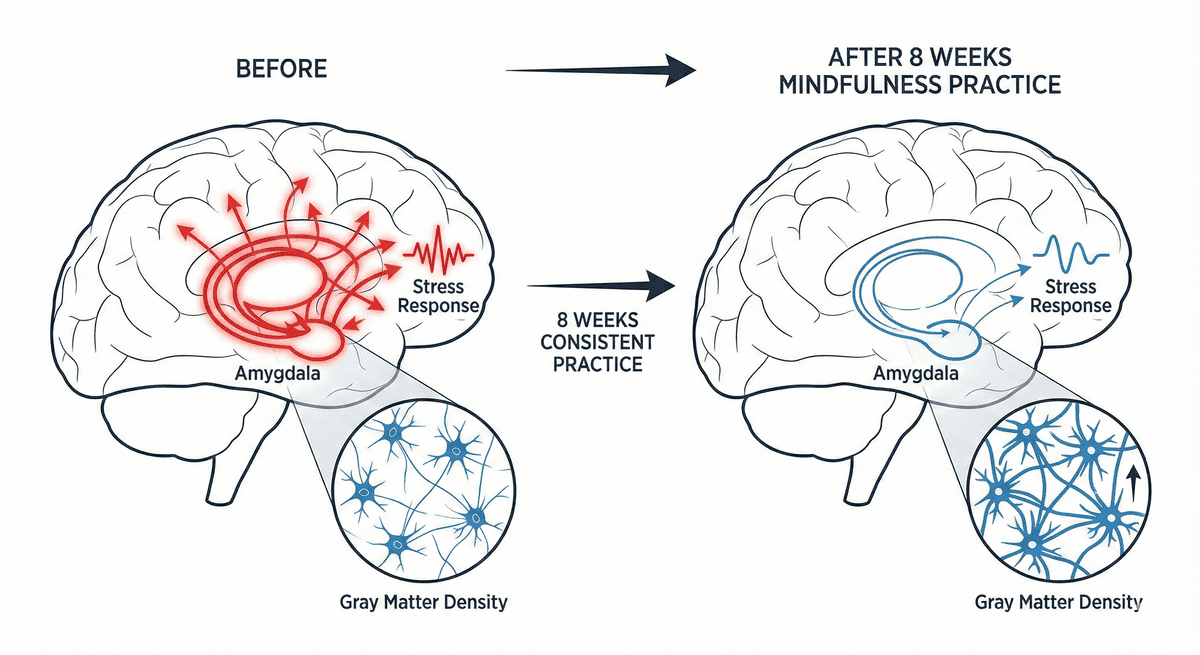
Amygdala Reactivity Reduction: Gray Matter Changes After Eight Weeks of Mindfulness Practice
Discover how eight weeks of mindfulness practice reshapes the brain, reducing amygdala reactivity and building lasting neural resilience.
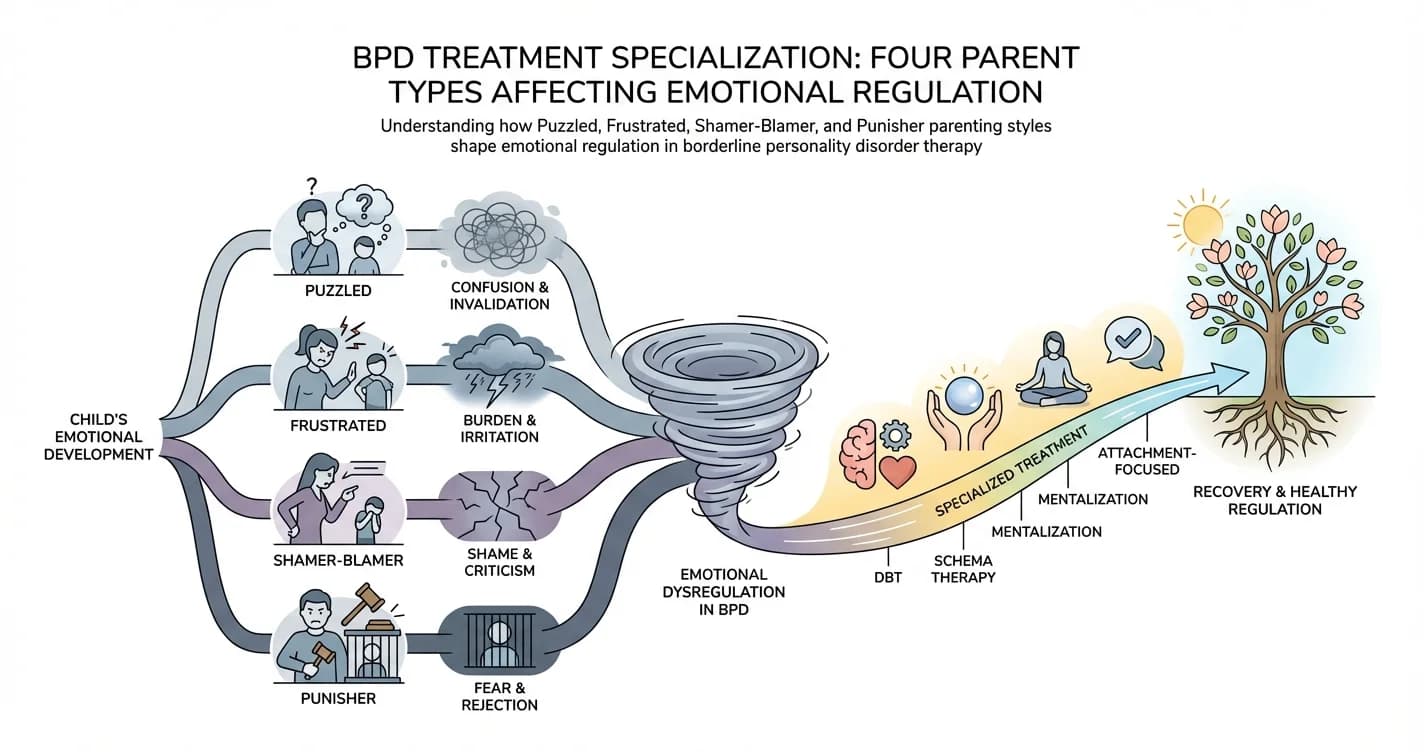
BPD Treatment Specialization: Four Parent Types Affecting Emotional Regulation
For individuals with borderline personality disorder (BPD), emotional regulation difficulties rarely emerge in isolation. Research increasingly suggests that
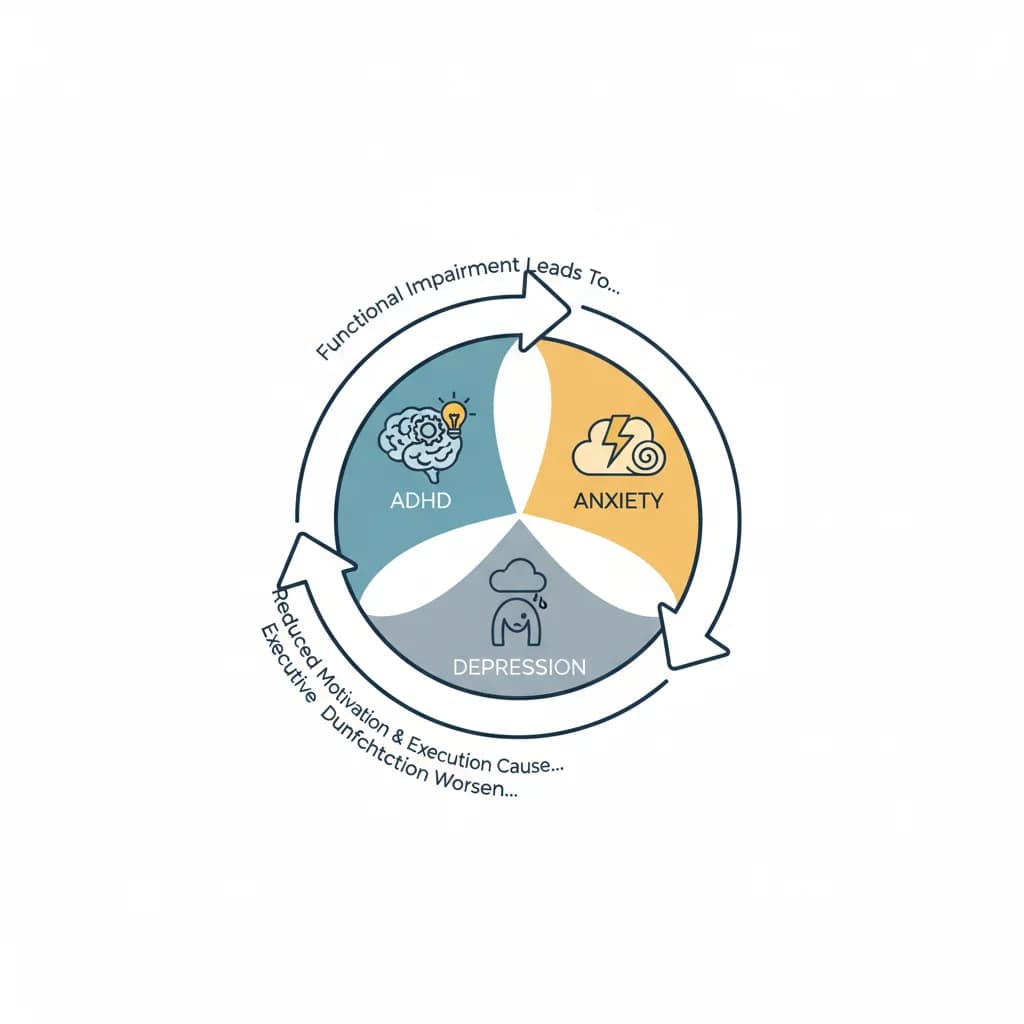
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.