Polyvagal Theory Explained: Stress & Safety (2026)
Polyvagal theory explained in plain language: learn the three nervous system states, what neuroception is, and how to regulate stress and anxiety in 2026.
Key Takeaways
- About 15 minutes of uninterrupted reading time
- A basic willingness to notice your own bodily sensations (no prior knowledge needed)
- Optionally: a journal to track which states you recognize in your own week
- No clinical background required — this guide uses plain language throughout
- Ventral vagal signs: steady breathing, easy eye contact, voice that sounds warm and modulated, genuine curiosity
Your nervous system is running an ancient threat-detection program right now — and polyvagal theory explains exactly how it works, why stress hijacks your body without permission, and what you can actually do about it.
TL;DR: Polyvagal theory, developed by neuroscientist Stephen Porges in 1994, describes three automatic nervous system states: the ventral vagal (safe and social), the sympathetic (fight-or-flight), and the dorsal vagal (shutdown/freeze). In 2026, this framework is one of the most cited models in trauma-informed therapy. Knowing which state you're in — and how to shift out of it — is the foundation of emotional regulation. This guide walks you through the theory step by step, with practical tools for each state.
Why this matters
Most people know stress feels bad. Fewer understand why their body freezes in an argument, why they can't calm down after a hard meeting, or why social connection is one of the fastest routes back to feeling okay. Polyvagal theory gives those experiences a name and a mechanism. Once you understand the three-state model, interventions that used to seem arbitrary — deep breathing, humming, cold water on your face — make immediate physiological sense.
What you'll need
- About 15 minutes of uninterrupted reading time
- A basic willingness to notice your own bodily sensations (no prior knowledge needed)
- Optionally: a journal to track which states you recognize in your own week
- No clinical background required — this guide uses plain language throughout
The three states: a quick map before the steps
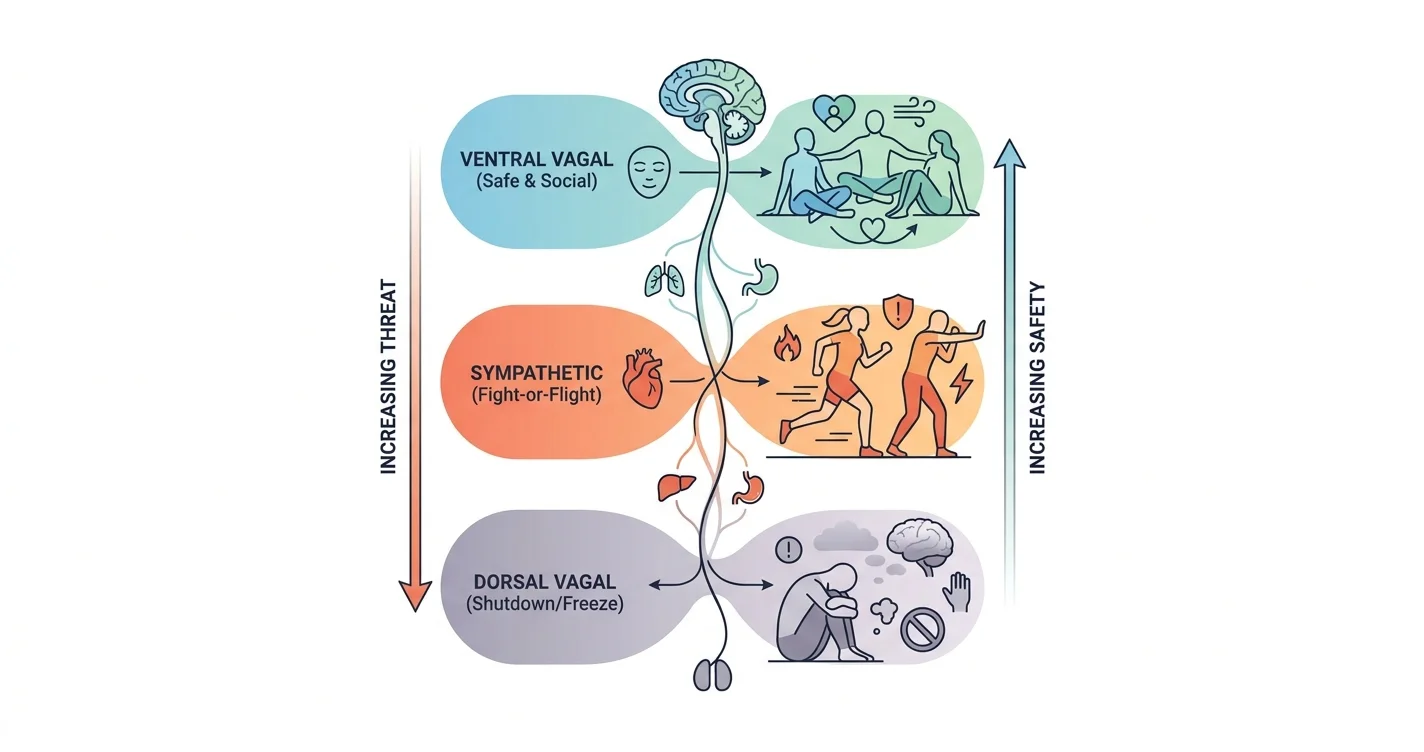
Polyvagal theory organizes the autonomic nervous system into three hierarchical circuits. They evolved in this order, and they activate in reverse order when threat increases.
| State | Circuit | What it feels like | Typical trigger |
|---|---|---|---|
| Ventral vagal | Social engagement | Calm, curious, connected | Safety cues from environment or people |
| Sympathetic | Fight-or-flight | Anxious, angry, restless | Perceived threat or danger |
| Dorsal vagal | Shutdown / freeze | Numb, collapsed, dissociated | Overwhelming or inescapable threat |
These aren't choices. They're automatic sequences your body runs based on incoming safety signals — what Porges calls neuroception, the nervous system's below-conscious threat scan.
Step 1 — Learn to identify your current state
Action: do a 60-second body check before you try to change anything.
You cannot regulate what you haven't named. The first step in applying polyvagal theory is recognizing which of the three states your nervous system is currently running.
- Ventral vagal signs: steady breathing, easy eye contact, voice that sounds warm and modulated, genuine curiosity
- Sympathetic signs: tight chest, racing heart, shallow breath, irritability, scanning the room, jaw tension
- Dorsal vagal signs: heavy limbs, foggy thinking, flatness in your voice, wanting to disappear, dissociation
A common mistake is labeling all bad feelings as "anxious" when shutdown and hyperarousal require opposite interventions. Stimulating a sympathetic-activated nervous system with cold exposure, for example, can backfire on someone already in dorsal collapse.
Expected outcome: You arrive at a working hypothesis — "I'm in sympathetic right now" — before choosing your next move.
Step 2 — Understand neuroception (the body's below-the-radar threat scan)
Action: stop blaming yourself for reactions you didn't consciously choose.
Neuroception is the process by which your nervous system evaluates risk 200–400 milliseconds before conscious awareness. Your brain registers a raised voice, a specific facial expression, or even a piece of music as safe or dangerous before you have a thought about it.
This is why you can feel dread in a "perfectly fine" meeting, or why a stranger's warm tone puts you at ease before you know anything about them. The nervous system is not reading the situation — it is reading signals: prosody (tone of voice), facial muscle movement, heart rate of people nearby, and environmental sounds in the low-to-mid frequency range.
In 2026, neuroception research continues to inform trauma therapy protocols, particularly somatic therapies and EMDR. The key implication is practical: your environment shapes your nervous system state continuously. You are not broken for having involuntary reactions. The system is doing its job.
Common mistake: Trying to think your way out of a sympathetic state. Cognition comes online after the body has already reacted. Start with the body first.
Step 3 — Work the ventral vagal anchor
Action: deliberately activate social engagement cues to signal safety.
The ventral vagal circuit — the newest evolutionary addition — runs through the face, voice, and middle ear. Activating it sends an "all clear" signal downward through the nervous system. Here is how to do that intentionally:
- Slow your exhale to twice the length of your inhale. A 4-count inhale and 8-count exhale activates the vagus nerve directly. Three cycles takes under 90 seconds.
- Hum or sing. Vibration in the throat stimulates the vagal tone. Even humming while exhaling counts.
- Make eye contact with a calm person. Co-regulation — borrowing another nervous system's calm — is one of the most efficient routes to a ventral vagal state. This is not a metaphor; it reflects mirror neuron activity and facial feedback loops.
- Listen to music with strong mid-range frequencies. Voices and instruments in the 500–2000 Hz range activate the middle ear muscles linked to the social engagement system.
Expected outcome: Reduced heart rate, a fuller breath, and a slight softening of facial muscles within 2–5 minutes.
Step 4 — Move through sympathetic activation, not around it
Action: discharge fight-or-flight energy physically before trying to calm down.
When your nervous system is in sympathetic activation, adrenaline and cortisol are already in your bloodstream. Telling yourself to calm down does not metabolize those hormones. Movement does.
- Shake your body for 60 seconds. Trauma researcher Peter Levine's somatic experiencing work documents how animals discharge stress through involuntary trembling after a threat passes. You can do this intentionally: stand and let your limbs shake loosely.
- Walk briskly for 10 minutes. Rhythmic, bilateral movement activates the prefrontal cortex and helps metabolize stress hormones faster.
- Push against a wall for 30 seconds. Isometric pressure gives the fight response somewhere to go.
This step is especially relevant if you notice the freeze response — sometimes what looks like shutdown is actually mobilized energy with nowhere to go, which benefits from gentle movement rather than stillness.
Common mistake: Trying to jump straight to meditation when your body is still flooded. Stillness during high sympathetic activation can intensify anxiety rather than reduce it.
Step 5 — Work back from dorsal vagal shutdown
Action: use micro-doses of gentle stimulation to resurface, not a shock to the system.
Dorsal vagal collapse — the freeze, the flatness, the "I can't" — is the nervous system's emergency brake. It is not laziness or depression (though it overlaps with depression neurologically). It is an ancient survival response to inescapable threat.
Coming back from dorsal shutdown requires graduated engagement, not forcing yourself to perform energy you don't have.
- Slow, rhythmic rocking. Self-rocking activates vestibular input and gently re-engages the ventral vagal circuit.
- Warm water or warmth on the face. Temperature change without shock stimulates the trigeminal nerve and nudges the system toward orientation.
- Name what you notice with curiosity, not judgment. "My hands feel heavy" is a grounding statement. It re-engages the prefrontal cortex without demanding a performance.
- Seek one low-demand connection. A text, a brief voice message, even a pet. Co-regulation is as effective here as in sympathetic states, but the dose matters — overwhelming social input can push a dorsal system deeper into collapse.
Expected outcome: Slight increase in energy, clearer thoughts, willingness to engage with small tasks. Full recovery from deep shutdown can take hours; do not measure progress in minutes.
Step 6 — Build a personal "nervous system map"
Action: track your state transitions for one week to find your patterns.
Polyvagal theory becomes genuinely useful when you stop applying it in crisis mode and start seeing your daily patterns. Use a simple journal format:
- Time of day
- State (ventral / sympathetic / dorsal)
- Trigger (person, environment, event, sound)
- What shifted it (if anything)
After 7 days, patterns emerge. Most people find 2–3 consistent triggers that push them into sympathetic activation and 1–2 people or environments that reliably return them to ventral vagal. That information is more useful than any generic tip list. In 2026, this kind of self-tracking is a core component of polyvagal-informed coaching and app-based mental health support.
Step 7 — Use the ladder daily, not just in emergencies
Action: practice ventral vagal state maintenance, not just recovery.
Porges uses the metaphor of a "ladder" — ventral vagal at the top, dorsal vagal at the bottom. Most people only think about the ladder when they've fallen off. Proactive maintenance means spending more baseline time in ventral vagal so the drop to sympathetic is shorter and the return is faster.
Daily practices that build ventral vagal tone over time (not just in the moment):
- 10 minutes of slow, paced breathing daily (4 in, 8 out)
- Regular physical contact or co-regulation with people or animals you feel safe with
- Minimizing chronic low-grade neuroceptive threats: loud open-plan offices, unpredictable social media scrolling, ambient news noise
- Consistent sleep — the vagal tone measurably decreases with fewer than 6 hours of sleep, based on heart rate variability data collected across multiple sleep studies through 2026
Troubleshooting
"I do the breathing but it doesn't calm me down." If you're in high sympathetic activation, breathing alone won't discharge adrenaline. Move first — walk, shake, push — then breathe.
"I can't tell which state I'm in." Start with two questions: Am I restless or collapsed? Restless points to sympathetic; collapsed points to dorsal. Pick your intervention from there.
"I feel worse when I try to meditate." Meditation without body awareness can amplify sympathetic activation for trauma-affected nervous systems. Ground the body first (feet on floor, feel weight in chair) before attempting stillness.
"My state changes within minutes and I can't keep up." Rapid state-switching is common with anxiety disorders and ADHD. The goal is not to stay perfectly ventral — it is to shorten the recovery window each time. Track length of episodes, not perfection.
"I know the theory but I can't apply it when I'm activated." This is the most common problem. Pre-set a single go-to intervention per state and practice it when you're calm. Muscle memory works; in-the-moment planning does not.
"My freeze response is happening a lot and I don't know why." Frequent dorsal activation often signals chronic relational or environmental threat — not a random malfunction. Exploring the fawn response and people-pleasing patterns may help identify what your nervous system is reacting to.
Tools and resources
- Journaling template: state / trigger / shift — run daily for 7 days
- Paced breathing: 4-count inhale, 8-count exhale, 3–5 minutes
- Movement protocol: 60-second shake or 10-minute bilateral walk for sympathetic discharge
- Reading: Stephen Porges, The Polyvagal Theory (2011) and The Pocket Guide to Polyvagal Theory (2017)
- Deb Dana, Polyvagal Exercises for Safety and Connection (2020) — the most accessible clinical workbook on applying this model
- Lovon — Lovon's AI voice therapy app guides users through nervous system regulation exercises and emotional check-ins in real time, drawing on frameworks including polyvagal-informed coping tools, available anytime without scheduling
- For deeper context on how the body responds to perceived threat, the amygdala hijack explainer covers the overlapping neuroscience in plain language
What to do next
Polyvagal theory explained the why — now the work is applying it. Start with Step 1 (the 60-second body check) every morning for one week before anything else. That single habit builds the interoceptive awareness that makes all the other tools land. If chronic sympathetic activation or freeze patterns are showing up in your relationships, that is worth exploring with a professional — Lovon can be a first step for daily support between sessions, not a replacement for clinical care when clinical care is what's needed.
FAQ
What is polyvagal theory in simple terms? Polyvagal theory describes three automatic states your nervous system cycles through — safe and social, fight-or-flight, and shutdown — based on how safe your environment feels. It was developed by Stephen Porges in 1994 and is now a core framework in trauma-informed therapy as of 2026.
What are the three states of polyvagal theory? Ventral vagal (calm, connected, socially engaged), sympathetic (anxious, activated, fight-or-flight), and dorsal vagal (collapsed, numb, frozen). Each state has a distinct set of physical sensations and behavioral patterns.
Is polyvagal theory scientifically proven? Polyvagal theory has strong empirical support for its clinical applications — particularly breathing-based vagal tone interventions and co-regulation — though some of its neuroanatomical claims remain debated in academic literature. It is widely applied in somatic therapy, EMDR, and trauma-informed care as of 2026.
How do I know if I'm in a dorsal vagal state? Common signs include emotional flatness, heavy limbs, foggy thinking, a monotone voice, and a strong pull toward withdrawal or isolation. It often feels like "nothing matters" rather than active fear.
Can you get stuck in fight-or-flight permanently? You cannot stay in sustained sympathetic activation indefinitely — the system eventually moves toward dorsal shutdown to conserve energy. Chronic stress, however, can create a pattern of oscillating between sympathetic and dorsal states with very little ventral vagal baseline.
How does polyvagal theory explain trauma? Trauma dysregulates the system's threat-detection threshold so that the nervous system reads neutral or safe situations as dangerous. Trauma-informed therapy works to expand the "window of tolerance" — the range of experience a person can stay present for while remaining in ventral vagal.
What is neuroception? Neuroception is the nervous system's automatic, below-conscious scan for safety or danger — it runs 200–400 milliseconds before your conscious mind has a thought. It explains why you can feel unsafe without being able to say why.
Does deep breathing actually work for anxiety? Yes, for specific reasons polyvagal theory makes clear: a long exhale activates the vagus nerve directly, which signals the heart to slow and pulls the system toward ventral vagal. The 4-count inhale, 8-count exhale ratio is the most researched pattern for this effect.
One last thing
The vagus nerve — the central cable of polyvagal theory — is the longest nerve in your body, running from your brainstem to your colon and touching your heart, lungs, and gut along the way. That is not metaphor; it is why gut feelings, heartache, and breathlessness under stress are real physical events, not figures of speech. Understanding that your body is not misbehaving — it is communicating — is often the most relieving thing a person learns from this framework.
Related guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
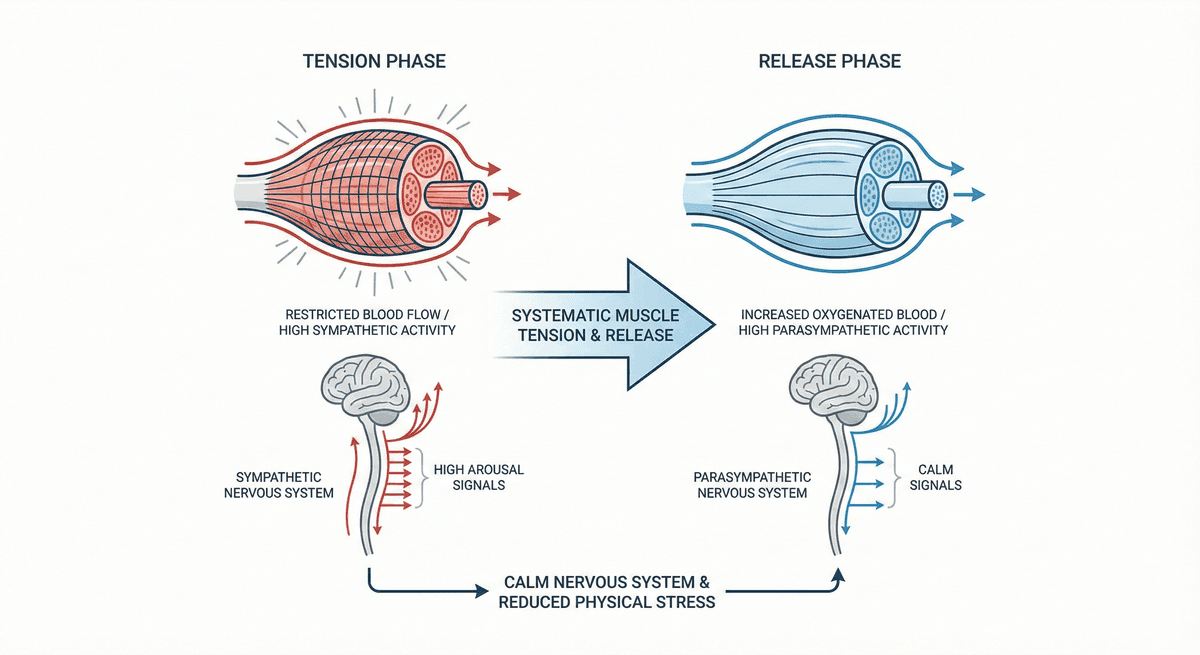
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.