OCPD vs OCD: Key Differences & Treatment (2026)
OCPD and OCD look similar but need different treatment. Learn the core differences, the ego-syntonic test, and the right therapy approach for each in 2026.
Key Takeaways
- A basic understanding of the DSM-5 criteria for both conditions (covered below)
- Awareness of whether the behaviors feel ego-syntonic (comfortable, self-consistent) or ego-dystonic (unwanted,
- Approximately 10 minutes to read this guide in full
- If you're supporting someone else, their willingness to discuss the topic
- Access to a licensed mental health professional for formal diagnosis — this guide informs, it does not diagnose
OCPD and OCD share three letters and a lot of surface-level overlap — both involve perfectionism, rigid rules, and repetitive behavior — but they are fundamentally different conditions that require different treatment paths. Getting the distinction right matters: misidentifying one as the other delays the right care by months or years.
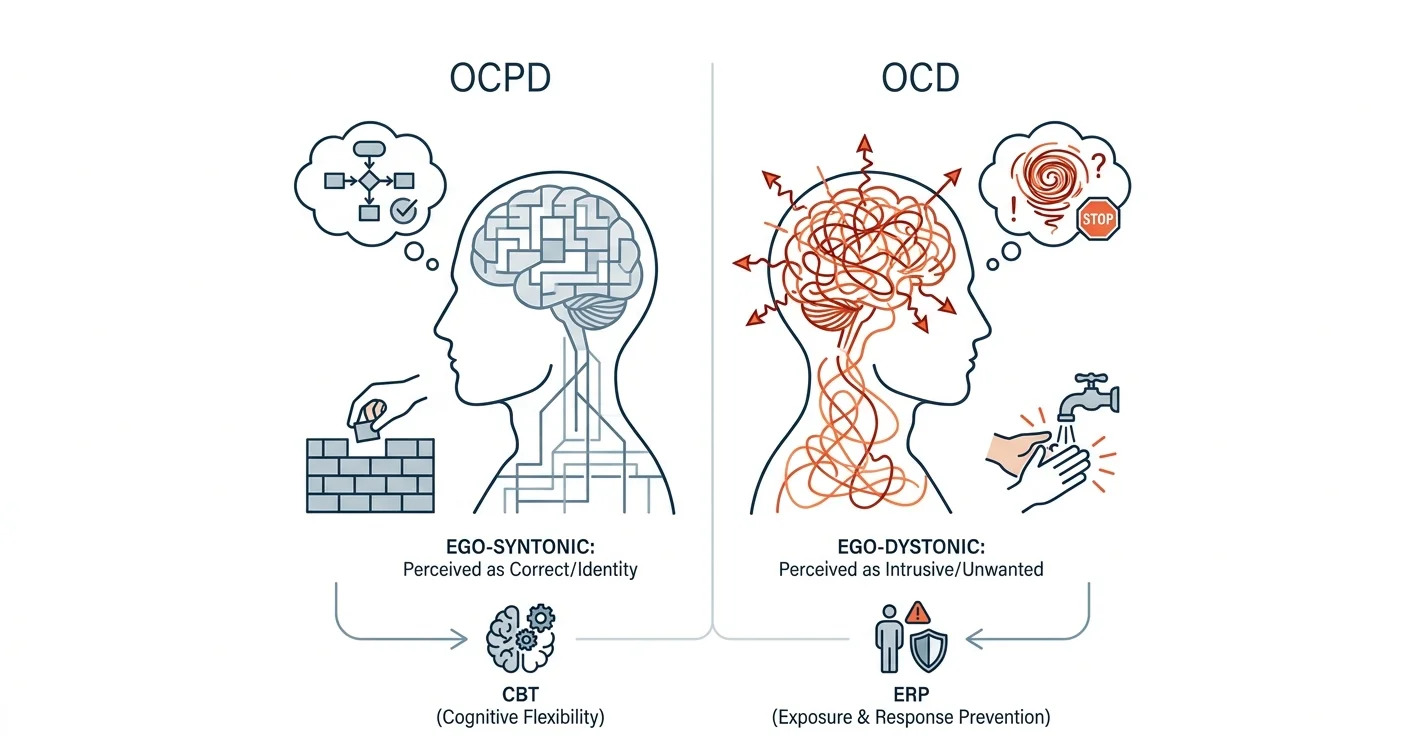
TL;DR: OCPD (Obsessive-Compulsive Personality Disorder) is a personality style where rigid perfectionism and control feel normal and correct to the person who has it. OCD (Obsessive-Compulsive Disorder) is an anxiety-driven cycle of intrusive thoughts and compulsions that the person recognizes as distressing and out of character. In 2026, the gold-standard treatment for OCD is ERP (Exposure and Response Prevention), while OCPD responds better to CBT focused on cognitive flexibility. They can co-occur in roughly 15–25% of OCD cases, which makes accurate diagnosis essential.
Why this matters
Both conditions are underdiagnosed and frequently confused — by patients, by family members, and occasionally by clinicians unfamiliar with personality disorder presentations. A person with OCPD rarely walks into a therapist's office saying "I have a problem." A person with OCD usually does. That single difference in self-perception drives everything downstream: how you recognize the condition, how you talk about it with a professional, and which therapeutic approach actually works.
What you'll need before you start
- A basic understanding of the DSM-5 criteria for both conditions (covered below)
- Awareness of whether the behaviors feel ego-syntonic (comfortable, self-consistent) or ego-dystonic (unwanted, distressing) — this is the key diagnostic dividing line
- Approximately 10 minutes to read this guide in full
- If you're supporting someone else, their willingness to discuss the topic
- Access to a licensed mental health professional for formal diagnosis — this guide informs, it does not diagnose
Step 1: Understand what each condition actually is
OCD is classified as an anxiety-related disorder in the DSM-5. It is defined by two core features: obsessions (recurring, intrusive, unwanted thoughts, images, or urges) and compulsions (repetitive mental or physical acts performed to reduce the distress those obsessions create). The person almost always knows the thoughts are excessive. They do not want them.
OCPD is a Cluster C personality disorder. It is a pervasive pattern of preoccupation with orderliness, perfectionism, and control — over both self and others — that begins in early adulthood and persists across most life situations. Crucially, people with OCPD typically believe their standards are correct and that other people are simply less disciplined. The behavior is not experienced as a disorder; it is experienced as identity.
The DSM-5 requires at least 4 of 8 criteria for an OCPD diagnosis. Common ones: rigid adherence to rules and lists, inability to delegate unless tasks are done exactly right, excessive devotion to work at the expense of relationships, inflexibility about ethics or values, and difficulty discarding worn-out objects.
Step 2: Apply the ego-syntonic vs. ego-dystonic test
This is the fastest practical filter.
- Ego-dystonic (OCD): "I know this thought is irrational but I can't stop it. The checking ritual feels awful but I can't not do it."
- Ego-syntonic (OCPD): "My way is the right way. If people followed the correct process, things would run smoothly."
Someone with OCD is typically distressed by their symptoms and wants relief. Someone with OCPD is typically distressed by other people's failure to meet their standards. That difference in the direction of distress is clinically significant and observable without any formal testing.
Step 3: Compare the specific behavioral patterns
| Feature | OCD | OCPD |
|---|---|---|
| Core driver | Anxiety from intrusive thoughts | Need for control and perfection |
| Insight | Usually aware thoughts are excessive | Typically believes standards are justified |
| Compulsions | Yes — ritualized, time-consuming | No true compulsions; more rule-following |
| Perfectionism | Possible, but tied to specific obsessions | Pervasive across all life domains |
| Impact on relationships | Person suffers; others may be confused | Others suffer from rigid expectations |
| Onset | Any age; often spikes in adolescence | Identifiable by early adulthood |
| Co-occurrence rate | OCPD present in ~15–25% of OCD cases | OCD present in a smaller subset of OCPD cases |
Three numbers worth holding onto: OCD affects approximately 2–3% of the US population over a lifetime. OCPD is the most prevalent personality disorder, estimated at 2–8% of the general population. When both are present simultaneously, the OCD tends to be more severe and harder to treat.
Step 4: Understand the treatment approach for OCD
Exposure and Response Prevention (ERP) is the first-line, evidence-based treatment for OCD as of 2026. ERP works by deliberately exposing the person to obsession-triggering situations and then preventing the compulsive response — allowing the anxiety to peak and naturally subside without the ritual reinforcing the cycle.
A typical ERP protocol runs 12–20 weekly sessions with a trained therapist. Response rates are strong: roughly 60–80% of people with OCD show clinically meaningful improvement with ERP. Selective serotonin reuptake inhibitors (SSRIs) are often used alongside ERP, particularly for moderate to severe presentations.
What does not work for OCD: talk therapy that focuses only on insight and understanding without behavioral exposure. Discussing the content of obsessions without the exposure component can actually strengthen them.
Step 5: Understand the treatment approach for OCPD
OCPD treatment is harder — not because the condition is more severe, but because the person rarely perceives themselves as the problem. The most effective approach is Cognitive Behavioral Therapy (CBT) targeting cognitive flexibility: challenging the all-or-nothing beliefs, the "should" statements, and the assumption that other people's methods are inherently inferior.
Schema therapy, which targets deep-seated belief patterns formed in childhood, has growing evidence for personality disorders including OCPD. Therapy for OCPD typically runs longer than OCD treatment — often 1–2 years — because personality patterns are more ingrained than symptom-specific anxiety cycles.
The entry point for someone with OCPD is often relationship distress: a partner, colleague, or family member reaches a breaking point. That external pressure sometimes creates enough motivation for the person to engage with therapy.
Step 6: Recognize what changes when both conditions are present
When OCD and OCPD co-occur, treatment planning shifts. The OCPD rigidity can actually interfere with ERP — people with high perfectionism sometimes turn ERP itself into a new rule-following compulsion rather than engaging with the genuine uncertainty the therapy requires. A skilled clinician will often address the OCPD cognitions first, or weave flexibility training into the ERP work.
If you or someone you know is navigating this combination, the priority is a thorough diagnostic evaluation that explicitly assesses both conditions rather than stopping at the more obvious OCD presentation.
Troubleshooting
"I check things repeatedly but it doesn't feel distressing — it just feels necessary." This pattern leans toward OCPD rather than OCD. The absence of distress about the behavior itself — as opposed to what happens if the behavior is interrupted — is a key signal. Bring this exact description to a clinician.
"My therapist is treating me for OCD but I'm not improving after 6 months of ERP." Poor ERP response sometimes indicates a co-occurring OCPD that hasn't been identified. Ask your therapist directly whether a personality disorder component has been evaluated.
"Someone told me perfectionism is always OCD." It is not. Perfectionism is a feature of several conditions — OCD, OCPD, eating disorders, anxiety disorders, and also high achievement without any disorder. The presence of perfectionism alone does not confirm either diagnosis.
"Can children be diagnosed with OCPD?" Not typically. DSM-5 requires that personality disorder traits be present across a long period and are not better explained by development. OCPD is generally diagnosable in late adolescence or early adulthood at the earliest.
"My partner insists they don't have a problem. How do I help?" You cannot diagnose or treat a partner. What you can do is name the impact on the relationship specifically and calmly — "When the kitchen has to be arranged this exact way, I feel like I can't live comfortably in our home" — and encourage couples or individual therapy. Lovon's AI therapy for anxiety and panic attacks resource covers anxiety-related coping tools that can also ease the distress of living with someone with rigid patterns.
"Is medication useful for OCPD?" No medications are FDA-approved specifically for OCPD. SSRIs are sometimes prescribed off-label for associated anxiety or depressive symptoms, but they do not address the core personality structure. Therapy is the primary treatment.
Tools and resources
- A licensed psychiatrist or psychologist for formal differential diagnosis — this is non-negotiable for conditions that overlap this closely
- Free AI therapist for anxiety — for managing day-to-day anxiety while pursuing formal evaluation or between therapy sessions
- The IOCDF (International OCD Foundation) maintains a therapist directory filtered by ERP training — iocdf.org
- Lovon's voice-based support for stress and burnout — useful when OCPD-related perfectionism is driving burnout symptoms
What to do next
If you've read this and still aren't sure which pattern fits, that uncertainty itself is useful information to bring to a clinician. Write down three specific behaviors that concern you, note whether each one feels distressing to you or primarily creates friction for others, and bring that list to an initial evaluation. That framing — ego-syntonic vs. ego-dystonic, not just a symptom checklist — will help a clinician move faster toward an accurate picture.
FAQ
What is the main difference between OCPD and OCD? OCD is an anxiety disorder driven by unwanted intrusive thoughts that the person finds distressing. OCPD is a personality disorder where rigid perfectionism and control feel normal and justified to the person who has it. The direction of distress is opposite: OCD sufferers are bothered by their own symptoms; people with OCPD are typically bothered by others not meeting their standards.
Can you have both OCD and OCPD at the same time? Yes. Research estimates that OCPD co-occurs in roughly 15–25% of OCD cases. When both are present, OCD symptoms tend to be more severe and ERP treatment is more complex, often requiring attention to OCPD's rigidity patterns alongside standard exposure work.
Does OCD always involve compulsions? Almost always. Pure obsessional OCD ("Pure O") still involves compulsions — they are often mental rather than physical, such as reviewing, reassuring, or neutralizing thoughts internally. The compulsion component is a defining feature of OCD in the DSM-5.
Is OCPD treatable? Yes, though treatment takes longer than OCD because it targets deep-seated personality patterns rather than specific symptom cycles. CBT focused on cognitive flexibility and schema therapy are the most evidence-supported approaches. Motivation to change is often the biggest barrier, since people with OCPD frequently do not see their behavior as a problem.
What triggers an OCD episode? OCD obsessions can be triggered by specific objects, situations, words, or images associated with the person's particular obsession theme (contamination, harm, symmetry, etc.). Stress and sleep deprivation reliably worsen OCD severity regardless of theme.
How long does OCD treatment take? A standard ERP protocol runs 12–20 weekly sessions. Many people see meaningful improvement within 3–4 months. Maintenance sessions or booster ERP may be needed during high-stress periods. OCPD treatment typically runs 1–2 years.
Can an app help with OCD or OCPD? Apps are not a substitute for ERP with a trained therapist for OCD, and they are not a treatment for OCPD. What AI-powered tools like Lovon can do is provide daily support between sessions — helping you process difficult feelings, practice grounding techniques, and reflect on patterns — which research on therapeutic homework suggests increases overall treatment outcomes.
When should someone with OCD see a psychiatrist vs. a psychologist? See a psychiatrist if medication evaluation is needed — particularly for moderate to severe OCD where SSRI augmentation is likely to help. See a psychologist or licensed therapist trained in ERP for the behavioral treatment itself. Ideally, both work together.
One last thing
OCPD is the most common personality disorder in the general population — more prevalent than borderline, narcissistic, or antisocial personality disorder combined — yet it receives a fraction of the clinical and public attention. Many people living with OCPD go decades without a diagnosis because their high achievement and rule-following often look, on the surface, like admirable traits. If the perfectionism in your life is costing you relationships or peace of mind rather than earning you both, that cost is worth examining.
Related guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
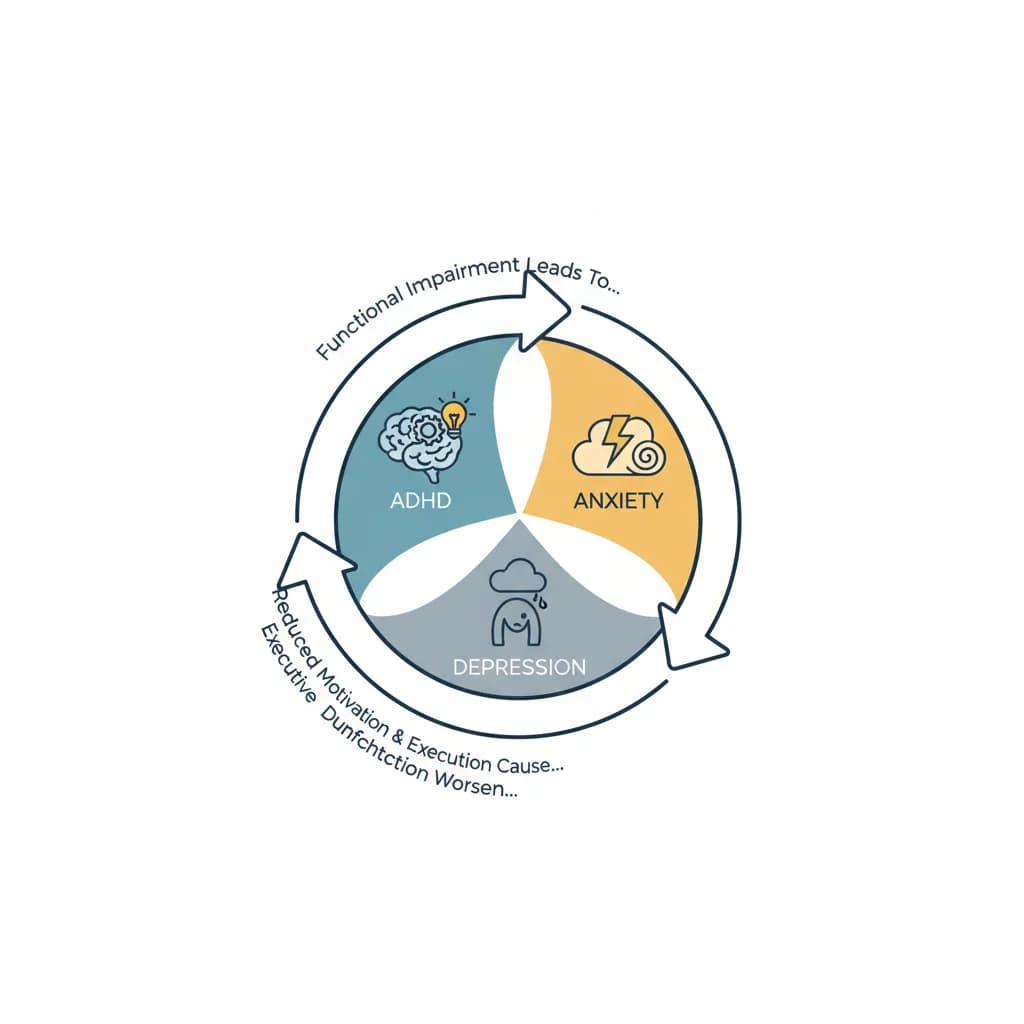
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
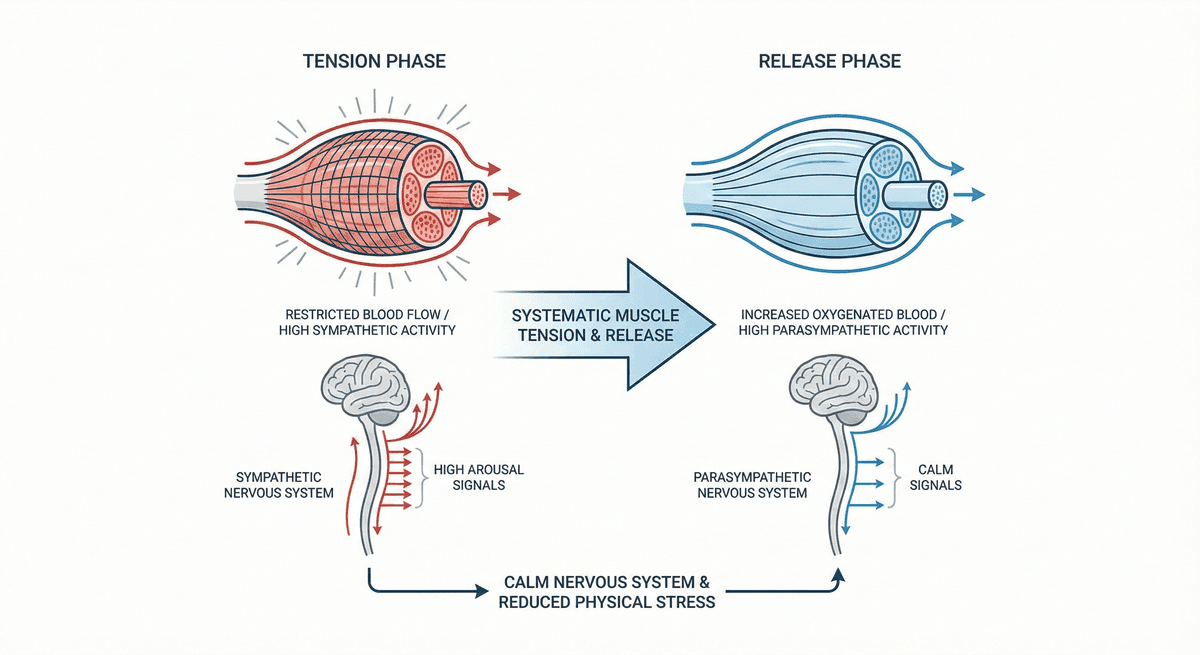
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
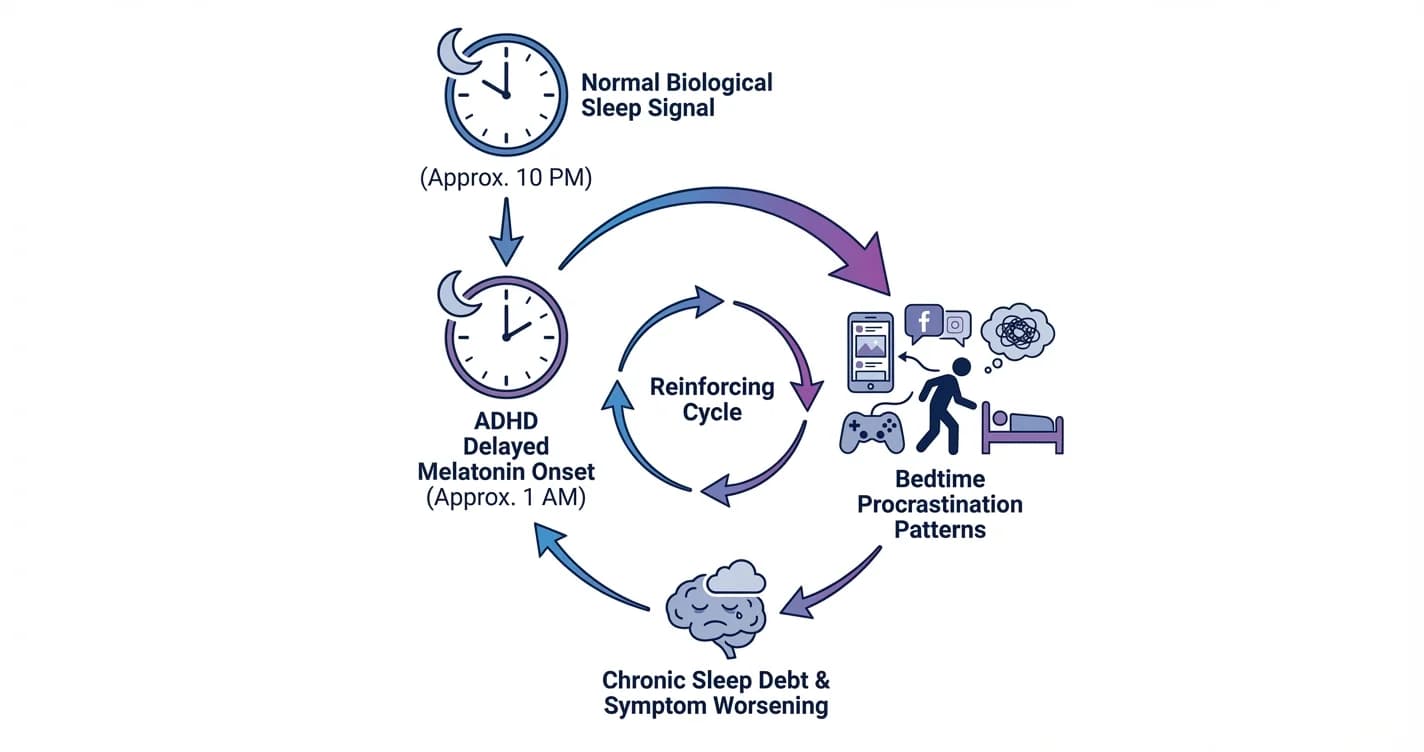
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.