Borderline Personality Disorder Crisis Management and Stigma Reduction
When someone with Borderline Personality Disorder (BPD) arrives at an emergency room in crisis, the situation is often misunderstood. What appears on the
Key Takeaways
- Intense emotional reactivity that feels uncontrollable to the person experiencing it
- Rapid escalation from baseline to crisis without apparent proportionality to triggers
- Physical symptoms including rapid heart rate, difficulty breathing, trembling, or dissociation
- Impaired ability to access logical thinking or remember coping strategies
- Heightened sensitivity to perceived rejection or abandonment cues
Introduction
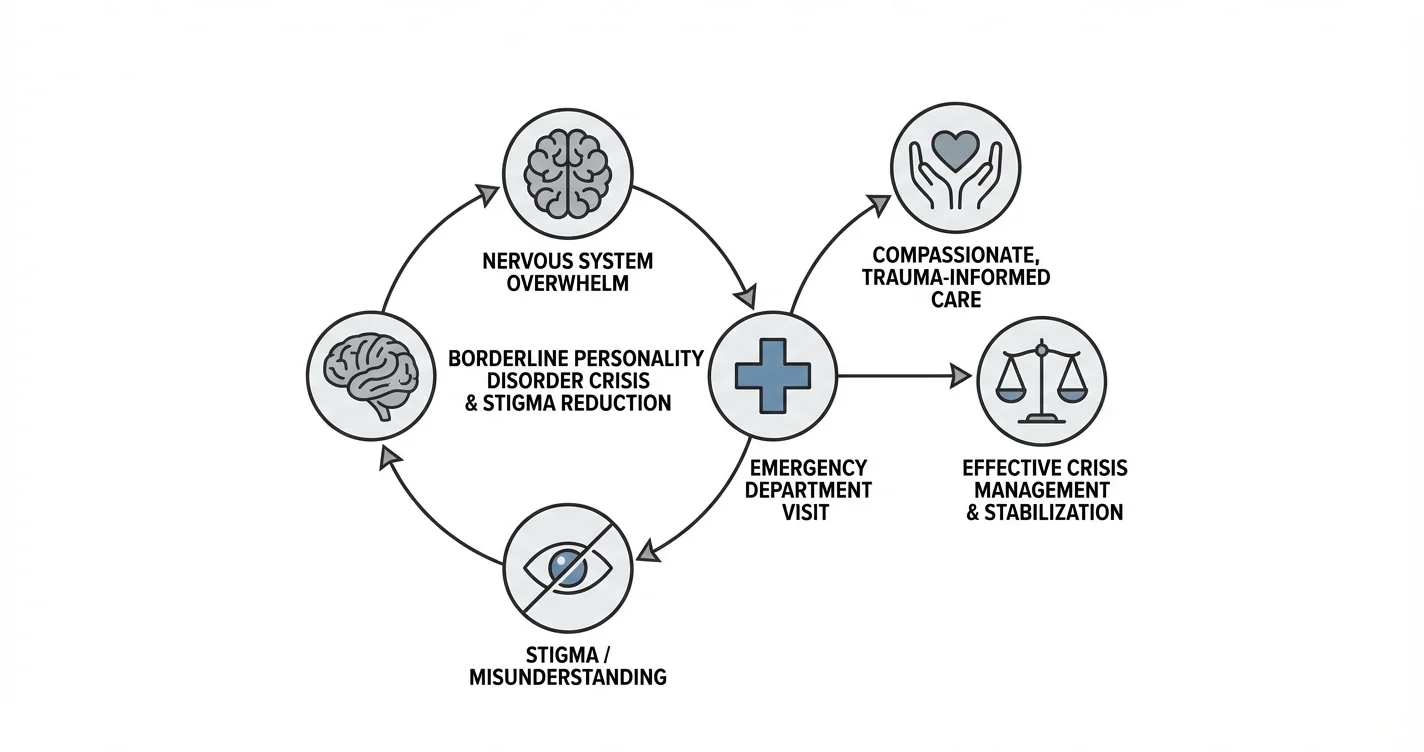
When someone with Borderline Personality Disorder (BPD) arrives at an emergency room in crisis, the situation is often misunderstood. What appears on the surface as dramatic behavior or attention-seeking may actually reflect profound nervous system overwhelm—a physiological response that has reached a tipping point. Borderline Personality Disorder crisis management requires understanding the biological realities of nervous system dysregulation, recognizing predictable crisis patterns, and addressing the pervasive stigma that affects care quality in emergency settings. This article draws on expert clinical insights and established research to provide practical guidance for individuals with BPD, their loved ones, and healthcare providers navigating these critical moments.
Understanding the interplay between nervous system stress, emergency department visits, and stigma reduction is essential for improving outcomes during BPD crises. Rather than viewing emergency visits as failures, recognizing them as opportunities for intervention can transform how care is delivered and received.
Understanding Nervous System Overwhelm in BPD Crises
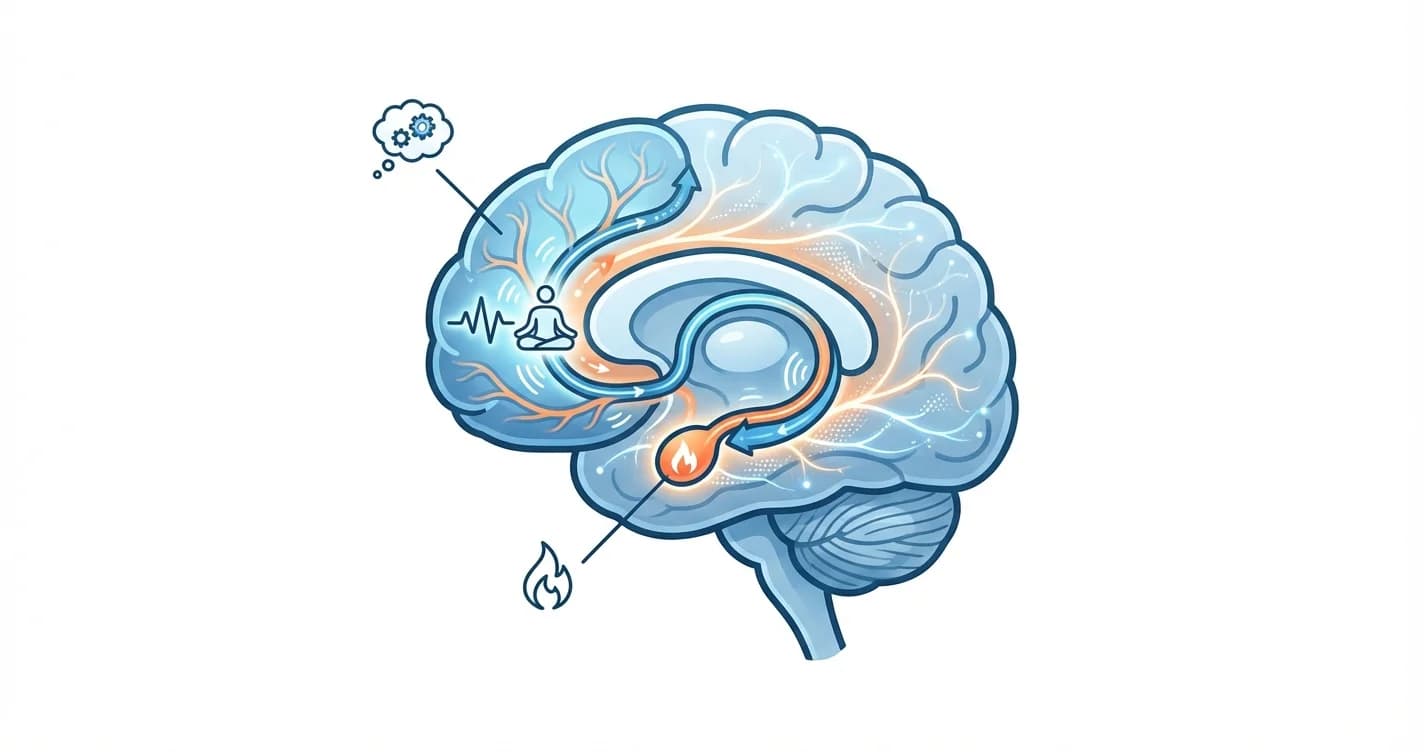
Borderline Personality Disorder involves significant difficulties with emotional regulation, which has clear neurobiological underpinnings. Research in affective neuroscience suggests that individuals with BPD may experience heightened sensitivity in brain regions associated with emotional processing, making intense emotional experiences more frequent and harder to modulate.
During a crisis, what clinicians observe is often a nervous system that has become completely overwhelmed. This is not a conscious choice or manipulative behavior—it reflects a physiological state where the body's stress response systems have exceeded their capacity to regulate. The autonomic nervous system, which governs our fight-flight-freeze responses, can become dysregulated to the point where rational thought and self-soothing become nearly impossible.
Key characteristics of nervous system overwhelm in BPD include:
- Intense emotional reactivity that feels uncontrollable to the person experiencing it
- Rapid escalation from baseline to crisis without apparent proportionality to triggers
- Physical symptoms including rapid heart rate, difficulty breathing, trembling, or dissociation
- Impaired ability to access logical thinking or remember coping strategies
- Heightened sensitivity to perceived rejection or abandonment cues
Clinical practitioners emphasize that these crisis episodes often follow predictable patterns for each individual. Understanding these patterns—what triggers them, how they escalate, and what typically helps—can be valuable information for crisis planning. However, during the overwhelm itself, the person experiencing it may have limited access to their usual cognitive resources.
Tools designed for immediate emotional processing, such as on-demand support platforms like Lovon.app, can provide accessible intervention points when someone notices early warning signs, potentially preventing escalation to full crisis.
Why Emergency Room Visits Occur During BPD Crises
Emergency department visits for Borderline Personality Disorder crises typically occur when someone experiences acute distress that feels unbearable or unsafe. These visits are often driven by specific circumstances that reflect genuine need rather than attention-seeking behavior—a distinction that is critical for reducing stigma.
Common reasons individuals with BPD present to emergency rooms include:
- Suicidal ideation or self-harm urges that feel overwhelming and difficult to manage safely alone
- Severe dissociative episodes where the person feels disconnected from reality or their own body
- Panic or anxiety that has reached intolerable levels, sometimes accompanied by physical symptoms mistaken for medical emergencies
- Inability to maintain safety when usual coping strategies have failed and support systems are unavailable
- Crisis following interpersonal conflict that triggers intense emotional pain and fears of abandonment
Studies examining psychiatric emergency department utilization indicate that individuals with personality disorders, including BPD, represent a significant proportion of repeat visits. However, this pattern reflects the chronic nature of emotional dysregulation rather than inappropriate use of services.
The challenge is that emergency departments are designed for acute medical crises and often lack the specialized resources needed for effective BPD crisis intervention. Emergency staff may have limited training in dialectical behavior therapy (DBT) techniques or trauma-informed approaches that are most effective for BPD. This mismatch between need and available resources contributes to poor experiences for both patients and providers.
When someone with BPD recognizes early signs of escalation—perhaps during a difficult evening or after a triggering interaction—having immediate access to emotional processing support can make the difference between managing the crisis at home and needing emergency services. Resources that offer real-time conversation and reflection, when accessed before full overwhelm occurs, may help interrupt the escalation cycle.
The Impact of Stigma on Borderline Personality Disorder Crisis Management
Stigma surrounding Borderline Personality Disorder in healthcare settings, particularly emergency rooms, represents a significant barrier to effective crisis management. Research on healthcare provider attitudes reveals that BPD is often viewed more negatively than other mental health conditions, with patients sometimes labeled as "difficult," "manipulative," or "attention-seeking."
This stigma manifests in several damaging ways during emergency department visits:
Dismissive treatment: When emergency staff view BPD crises as behavioral rather than genuine medical emergencies, patients may receive minimal intervention or be discharged prematurely without adequate safety planning.
Delayed or withheld care: Some individuals with BPD report long wait times or providers who are reluctant to engage meaningfully with their distress, creating a paradox where seeking help becomes another source of trauma.
Inadequate assessment: Stigma can lead to cursory evaluations that miss important safety concerns or fail to differentiate between chronic suicidal ideation and acute risk elevation.
Self-fulfilling cycles: When patients sense judgment or dismissiveness, their distress may escalate, confirming provider biases about "difficult" behavior and reinforcing negative attitudes.
Experts emphasize that understanding the neurobiological basis of BPD symptoms—recognizing that nervous system overwhelm is a physiological reality—can help reduce stigma. When providers frame BPD crises as legitimate medical emergencies involving dysregulated stress response systems rather than character flaws, care quality improves substantially.
Stigma reduction also requires systemic changes, including specialized training for emergency department staff in personality disorders, implementation of trauma-informed care principles, and development of crisis response protocols specifically designed for emotional dysregulation.
For individuals with BPD, anticipating potential stigma and preparing for emergency visits can help. This might include bringing a crisis plan that outlines effective interventions, having a trusted support person who can advocate if needed, and requesting providers trained in DBT or BPD-specialized approaches when possible.
Practical Strategies for Managing BPD Crises
Effective Borderline Personality Disorder crisis management involves both preventive strategies and interventions during acute episodes. Clinical experts recommend a multi-layered approach that addresses crises at different stages of escalation.
Early Intervention and Prevention
The most effective crisis management happens before full nervous system overwhelm occurs. Recognizing early warning signs—changes in sleep, increased sensitivity to perceived slights, subtle shifts in emotional intensity—allows for earlier intervention.
Grounding techniques are fundamental tools recommended by practitioners specializing in BPD treatment. These include sensory-based strategies like holding ice, focused breathing exercises, and progressive muscle relaxation. While these may seem simple, they work by engaging the parasympathetic nervous system, which can help counteract escalating stress responses.
Predictable crisis patterns can be mapped and anticipated. Many individuals with BPD notice that crises follow certain triggers or occur during specific circumstances (late evening, after certain types of interactions, during transitions). Identifying these patterns allows for increased vigilance and preemptive use of coping strategies during high-risk times.
Accessible support options play a crucial role in early intervention. Being able to process emerging distress through conversation—whether with a therapist, crisis line, trusted friend, or through platforms like Lovon.app that offer on-demand emotional processing—can prevent escalation by providing reflection and validation during the critical window before overwhelm.
During Acute Crisis
When someone is in the midst of a BPD crisis with significant nervous system overwhelm, interventions need to be simple and focused on immediate safety and stabilization rather than complex problem-solving.
Safety first: If there is immediate risk of self-harm or suicide, emergency services should be contacted. Having a pre-established crisis plan that outlines who to call and what has helped in the past can streamline this process.
Simplify communication: During overwhelming distress, complex conversations or problem-solving attempts often backfire. Brief, validating statements ("I see this is incredibly difficult," "We'll get through this moment together") work better than trying to rationalize or fix the situation.
Physical comfort and presence: For some individuals, supportive physical presence (if welcome) or creating a calm, safe physical environment helps more than verbal interventions. This might include dim lighting, comfortable temperature, minimal stimulation.
Avoid judgment or dismissiveness: Whether from emergency providers, family members, or the individual themselves, judgmental responses typically intensify distress. Treating the crisis as legitimate and deserving of compassionate response is essential.
After the Crisis
Post-crisis reflection is valuable for improving future crisis management. When the acute episode has passed and the nervous system has settled, reviewing what happened, what triggered it, and what helped or didn't help can inform future crisis planning.
This is also an appropriate time to work with a therapist specializing in BPD (particularly those trained in DBT or mentalization-based therapy) to strengthen emotional regulation skills and address underlying patterns. Professional support is essential for long-term management, though it complements rather than replaces the immediate coping strategies used during acute episodes.
When to Seek Professional Help
While self-management strategies and support resources are valuable, certain situations require professional intervention. Individuals with BPD should seek immediate professional help when:
- Experiencing thoughts of suicide or specific plans to harm themselves
- Unable to maintain physical safety or having strong urges to engage in life-threatening self-harm
- Experiencing complete disconnection from reality or severe dissociative episodes
- Finding that crises are increasing in frequency or intensity despite using coping strategies
- Noticing significant functional impairment—inability to work, maintain relationships, or care for basic needs
Professional help for BPD typically involves therapists specializing in evidence-based treatments including Dialectical Behavior Therapy (DBT), mentalization-based therapy, or schema-focused therapy. Psychiatrists can evaluate whether medications might help with specific symptoms such as mood instability or anxiety, though medication is generally considered adjunctive to therapy for BPD.
For crisis situations, options include:
- Crisis lines that provide immediate telephone support (988 Suicide & Crisis Lifeline in the US)
- Mobile crisis teams in some areas that can come to your location
- Psychiatric emergency services or emergency departments when immediate safety evaluation is needed
- Crisis stabilization units that offer short-term intensive support as an alternative to hospital admission
Having a relationship with a therapist who specializes in BPD provides continuity of care and someone who understands your specific patterns, which can make crisis episodes more manageable and less likely to require emergency services.
Conclusion
Borderline Personality Disorder crisis management becomes more effective when we understand that emergency room visits and acute episodes often reflect genuine nervous system overwhelm rather than attention-seeking behavior. Recognizing the neurobiological reality of emotional dysregulation, implementing grounding techniques during early escalation, and having accessible support options can prevent many crises from reaching the point where emergency services are needed.
Stigma reduction in healthcare settings—particularly emergency departments—requires both education about the physiological basis of BPD symptoms and systemic implementation of trauma-informed, compassionate care protocols. When individuals with BPD receive understanding and appropriate intervention during crises, outcomes improve significantly.
For those living with Borderline Personality Disorder, developing personalized crisis management strategies, including identification of early warning signs and accessible support resources, creates a foundation for navigating difficult moments more safely. Whether through professional therapy, crisis planning, or on-demand support tools, having multiple layers of intervention available increases resilience and reduces the intensity and frequency of crises over time.
Disclaimer: This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm—seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
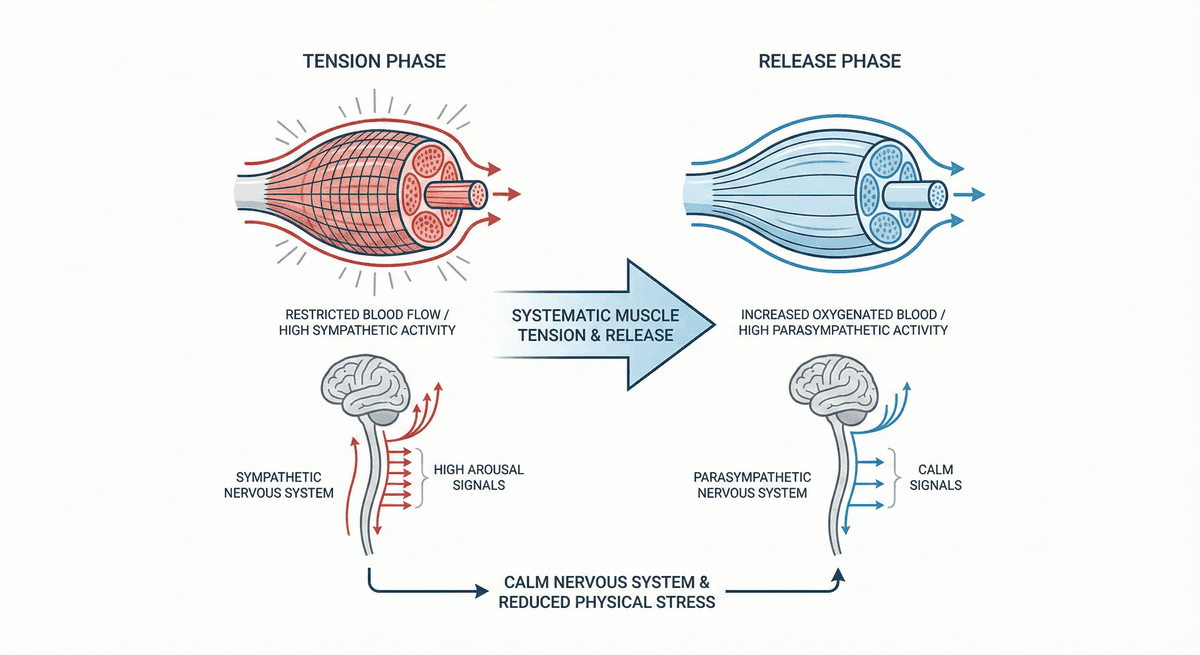
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.