PTSD vs CPTSD — Symptom Categories and Trauma Exposure Patterns
When someone experiences trauma, the psychological impact can manifest in different ways depending on the nature and duration of the traumatic exposure.
Key Takeaways
- Combat experiences or exposure to warfare
- Natural disasters such as earthquakes, floods, or hurricanes
- Serious motor vehicle accidents
- Physical or sexual assault (single incident)
- Witnessing violence or death
Introduction
When someone experiences trauma, the psychological impact can manifest in different ways depending on the nature and duration of the traumatic exposure. Understanding the difference between PTSD vs CPTSD — symptom categories and trauma exposure patterns — is essential for recognizing how these conditions develop and what distinguishes them from one another. While both post-traumatic stress disorder (PTSD) and complex post-traumatic stress disorder (CPTSD) arise from traumatic experiences, they reflect fundamentally different patterns of trauma exposure and produce distinct symptom clusters. Research suggests that PTSD typically develops following discrete traumatic events, while CPTSD emerges from prolonged, repeated trauma often occurring in circumstances where escape feels impossible. This article examines the specific symptom categories that characterize each condition and explores how different trauma exposure patterns contribute to their development.
Understanding the Core Distinction Between PTSD and CPTSD
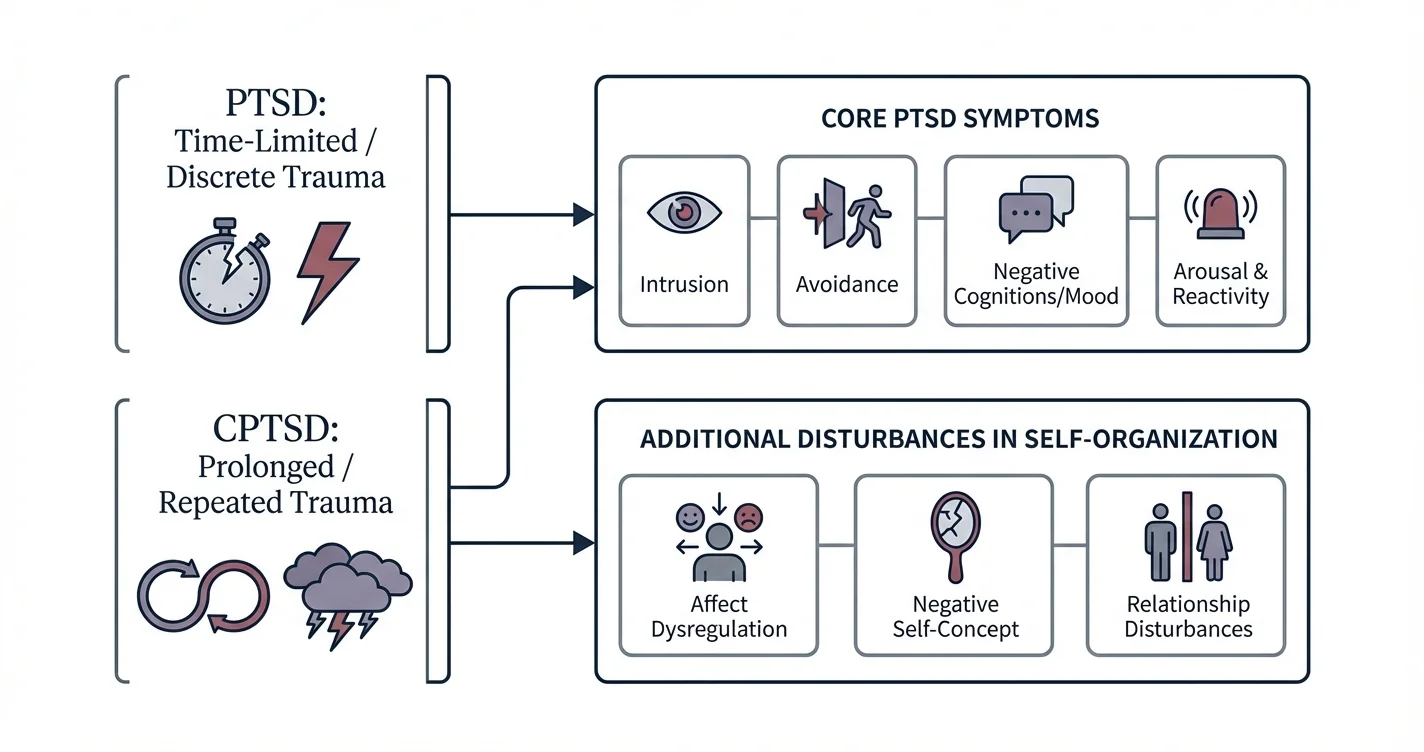
The fundamental difference between PTSD and CPTSD lies not only in the severity of symptoms but in the qualitative nature of both the trauma exposure and the resulting psychological impact. PTSD was originally conceptualized to describe the psychological aftermath of discrete traumatic events — such as combat exposure, natural disasters, serious accidents, or single-incident assaults. The diagnostic framework focuses on intrusion symptoms, avoidance behaviors, negative alterations in cognition and mood, and changes in arousal and reactivity.
CPTSD, recognized more recently in the International Classification of Diseases (ICD-11), encompasses all the core PTSD symptoms but adds three additional symptom clusters that reflect deeper disruptions in psychological functioning. These additional domains include disturbances in self-organization: difficulties with emotion regulation, negative self-concept, and disturbances in relationships. Clinical research indicates that these additional symptoms emerge specifically from prolonged trauma exposure, particularly when that trauma occurs in contexts involving interpersonal betrayal, captivity, or during critical developmental periods.
The distinction matters considerably for treatment approaches. While evidence-based treatments for PTSD focus primarily on processing traumatic memories and addressing specific fear responses, treatment approaches for CPTSD must additionally address fundamental difficulties in emotional regulation, identity, and interpersonal functioning that developed as adaptations to chronic traumatic environments.
Trauma Exposure Patterns: Single-Event vs Prolonged Trauma
The type and duration of trauma exposure represents one of the clearest differentiators when comparing PTSD and CPTSD symptoms and types of trauma exposure. PTSD typically develops following traumatic events that, while potentially devastating, are time-limited. These might include:
- Combat experiences or exposure to warfare
- Natural disasters such as earthquakes, floods, or hurricanes
- Serious motor vehicle accidents
- Physical or sexual assault (single incident)
- Witnessing violence or death
- Life-threatening medical events
In contrast, CPTSD emerges from prolonged, repeated traumatic experiences, particularly those involving interpersonal trauma where the individual cannot easily escape. Common trauma exposure patterns associated with CPTSD include:
- Childhood abuse (physical, sexual, or emotional) occurring over months or years
- Prolonged domestic violence in adult relationships
- Human trafficking or captivity situations
- Prolonged childhood neglect or emotional unavailability from caregivers
- Being held as a prisoner of war or in concentration camps
- Systematic torture or political imprisonment
- Cult involvement with coercive control
Research suggests that the chronicity and inescapability of these situations fundamentally alter how the individual develops psychological coping mechanisms. When trauma becomes the norm rather than the exception, individuals may develop persistent alterations in their sense of self, their ability to regulate emotions, and their capacity to form trusting relationships. These adaptations, while protective during the traumatic circumstances, become the additional symptom clusters that distinguish CPTSD from PTSD.
The developmental timing of trauma exposure also matters significantly. When prolonged trauma occurs during childhood — particularly during critical periods of brain development and identity formation — it can disrupt normal developmental processes related to attachment, self-concept formation, and emotional regulation capacity.
Symptom Categories: Core PTSD Features
When examining symptom categories and trauma patterns in PTSD compared to CPTSD, it's essential to first understand the core symptom clusters that define PTSD itself. These symptoms typically emerge following the traumatic event and persist for more than one month, causing significant distress or functional impairment.
Intrusion Symptoms represent involuntary re-experiencing of the traumatic event through:
- Recurrent, intrusive distressing memories of the trauma
- Nightmares with content related to the traumatic event
- Flashback episodes where the person feels as if the trauma is recurring
- Intense psychological distress when exposed to trauma reminders
- Physical reactions (increased heart rate, sweating) to trauma cues
Avoidance Behaviors involve persistent efforts to avoid trauma-related stimuli:
- Avoiding thoughts, feelings, or conversations about the trauma
- Avoiding people, places, activities, or situations that trigger trauma memories
- Inability to recall important aspects of the traumatic event (dissociative amnesia)
Negative Alterations in Cognitions and Mood include:
- Persistent negative beliefs about oneself, others, or the world ("I am bad," "No one can be trusted")
- Distorted blame of self or others for causing the trauma or its consequences
- Persistent negative emotional states (fear, horror, anger, guilt, shame)
- Diminished interest in previously enjoyed activities
- Feelings of detachment from others
- Inability to experience positive emotions
Alterations in Arousal and Reactivity manifest as:
- Irritable behavior or angry outbursts
- Reckless or self-destructive behavior
- Hypervigilance (being constantly "on guard")
- Exaggerated startle response
- Concentration difficulties
- Sleep disturbances
These core symptoms reflect the brain and body's ongoing response to perceived threat, even when the actual danger has passed. Neuroimaging studies suggest that PTSD involves altered functioning in brain regions associated with threat detection, fear conditioning, and emotional regulation, including the amygdala, hippocampus, and prefrontal cortex.
Additional Symptom Categories Specific to CPTSD
The symptom and trauma pattern differences between PTSD and CPTSD become particularly apparent when examining the three additional symptom domains that define CPTSD. These "disturbances in self-organization" reflect the profound impact of prolonged trauma on core aspects of psychological functioning.
Affect Dysregulation in CPTSD goes beyond the emotional numbing or reactivity seen in PTSD. It involves:
- Heightened emotional reactivity with difficulty returning to emotional baseline
- Emotional responses that feel overwhelming and uncontrollable
- Difficulty identifying and describing emotional states
- Rapid shifts between emotional states
- Tendency toward emotional shutdown or numbness when overwhelmed
- Using potentially harmful behaviors to manage emotions (substance use, self-harm)
People with CPTSD often describe feeling like their emotions "hijack" them, leading to responses that feel disproportionate to current situations. This reflects the fact that prolonged trauma during development can interfere with learning healthy emotion regulation strategies. Tools designed to provide on-demand support, such as Lovon.app, can offer accessible options for processing emotional experiences between therapy sessions, helping individuals practice putting words to overwhelming feelings.
Negative Self-Concept represents persistent and pervasive negative beliefs about oneself:
- Feelings of being permanently damaged, defeated, or worthless
- Deep shame about oneself (not just about specific actions)
- Sense of being fundamentally different from others
- Beliefs about being deserving of bad treatment
- Feeling permanently changed or contaminated by the trauma
This differs from the negative cognitions in PTSD, which tend to be more specifically connected to the traumatic event itself. In CPTSD, the negative self-concept becomes a core part of identity rather than a trauma-specific belief.
Disturbances in Relationships manifest as persistent difficulties across interpersonal contexts:
- Difficulty feeling close to others or trusting people
- Tendency to avoid relationships altogether
- Pattern of remaining in harmful relationships
- Difficulty maintaining consistent relationship patterns
- Feeling disconnected from others even in close relationships
- Oscillating between desperate clinging and complete withdrawal
These relationship disturbances emerge logically from trauma histories where other people were the source of harm, particularly during developmental periods when attachment patterns form. When caregivers who should provide safety instead provide threat, individuals may develop contradictory working models of relationships that persist into adulthood.
Recognizing Overlapping and Distinct Features in Clinical Presentation
When clinicians assess how PTSD and CPTSD differ in symptom types and trauma exposure, they look for both overlapping features and distinctive patterns. Both conditions share the core PTSD symptom clusters, but CPTSD additionally involves the pervasive difficulties with self-regulation, self-concept, and relationships that developed through prolonged trauma exposure.
Some individuals may experience symptoms that fall along a continuum between the two conditions. Factors that influence whether someone develops PTSD versus CPTSD following trauma include:
- Duration and frequency of traumatic exposure
- Age at which trauma occurred (earlier onset often associated with more complex presentations)
- Relationship to the perpetrator (interpersonal trauma, especially by caregivers, increases CPTSD risk)
- Presence of protective factors (supportive relationships, periods of safety)
- Genetic predispositions and individual temperament
- Access to support and intervention during or after trauma
It's important to recognize that neither condition reflects personal weakness or failure. Both represent understandable psychological responses to overwhelming experiences. While early experiences and trauma exposure play significant roles in these conditions, genetic factors and individual temperament also contribute to how these patterns develop and manifest.
Treatment Implications and Approaches
Understanding the difference between PTSD and CPTSD symptom categories and trauma patterns directly informs treatment planning. For PTSD, evidence-based treatments typically include:
- Trauma-focused cognitive behavioral therapy (TF-CBT)
- Eye Movement Desensitization and Reprocessing (EMDR)
- Prolonged Exposure (PE) therapy
- Cognitive Processing Therapy (CPT)
These approaches focus primarily on processing traumatic memories, addressing avoidance patterns, and modifying trauma-related beliefs.
For CPTSD, treatment generally requires a phased approach that addresses the additional symptom clusters:
Phase 1: Stabilization and Safety focuses on:
- Establishing current safety and addressing ongoing threats
- Developing emotion regulation skills
- Building distress tolerance strategies
- Establishing therapeutic relationship and trust
Phase 2: Trauma Processing involves:
- Gradually processing traumatic memories
- Integrating fragmented aspects of experience
- Addressing trauma-related beliefs and meanings
Phase 3: Integration and Reconnection emphasizes:
- Developing more coherent sense of identity
- Building relationship skills and healthy connections
- Establishing meaningful life direction
Research suggests that attempting intensive trauma processing too early with CPTSD, before adequate emotion regulation skills are established, can potentially lead to destabilization. This reflects the practical reality that individuals with CPTSD may have fewer internal resources for managing the distress that trauma processing can initially generate.
Between formal therapy sessions, individuals may benefit from accessible support options for processing emotions and working through daily stressors. On-demand resources can complement professional treatment by providing space to talk through challenges as they arise, helping to bridge the gaps between scheduled appointments.
When to Seek Professional Help
If you recognize symptoms of either PTSD or CPTSD affecting your daily functioning, relationships, or well-being, seeking professional support is an important step. Consider reaching out to a mental health professional if you experience:
- Intrusive memories, flashbacks, or nightmares that interfere with daily life
- Persistent avoidance of people, places, or activities due to trauma associations
- Overwhelming emotions that feel uncontrollable or lead to harmful behaviors
- Persistent negative beliefs about yourself as fundamentally damaged or worthless
- Difficulty maintaining relationships or ongoing patterns of relationship conflict
- Hypervigilance, sleep disturbances, or concentration problems affecting work or functioning
- Thoughts of self-harm or suicide
Mental health professionals who specialize in trauma treatment — including psychologists, psychiatrists, licensed clinical social workers, and counselors with trauma-specific training — can conduct thorough assessments and develop appropriate treatment plans. For CPTSD specifically, seeking providers with experience in complex trauma and phase-based treatment approaches may be particularly beneficial.
Treatment approaches can vary considerably between individuals, and what works for one person may need adaptation for another. Professional guidance helps ensure that interventions match your specific symptom presentation, trauma history, and current resources.
Conclusion
The distinction between PTSD vs CPTSD — symptom categories and trauma exposure patterns — reflects important differences in both the nature of traumatic experiences and their psychological impacts. PTSD typically emerges from discrete traumatic events and involves intrusion symptoms, avoidance, negative cognitions and mood, and altered arousal. CPTSD encompasses these core features but adds pervasive difficulties with emotion regulation, negative self-concept, and relationship disturbances that emerge specifically from prolonged, repeated trauma, particularly during developmental periods or in contexts involving interpersonal betrayal and inescapability.
Understanding these differences matters not only for accurate recognition but for accessing appropriate treatment approaches. While PTSD treatment focuses primarily on trauma memory processing, CPTSD treatment requires additional attention to stabilization, emotion regulation skill development, and rebuilding fundamental capacities for self-regulation and connection. Both conditions represent understandable responses to overwhelming experiences, and both can improve significantly with appropriate support and treatment. If you recognize these patterns in your own experience, reaching out to a trauma-informed mental health professional represents an important step toward recovery and integration.
Disclaimer: This is general information, not medical advice or diagnosis. If symptoms are severe, affecting your daily life, or you're having thoughts of self-harm — seek professional help. In the US: call or text 988 (Suicide & Crisis Lifeline). For immediate danger: 911 or local emergency services.
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
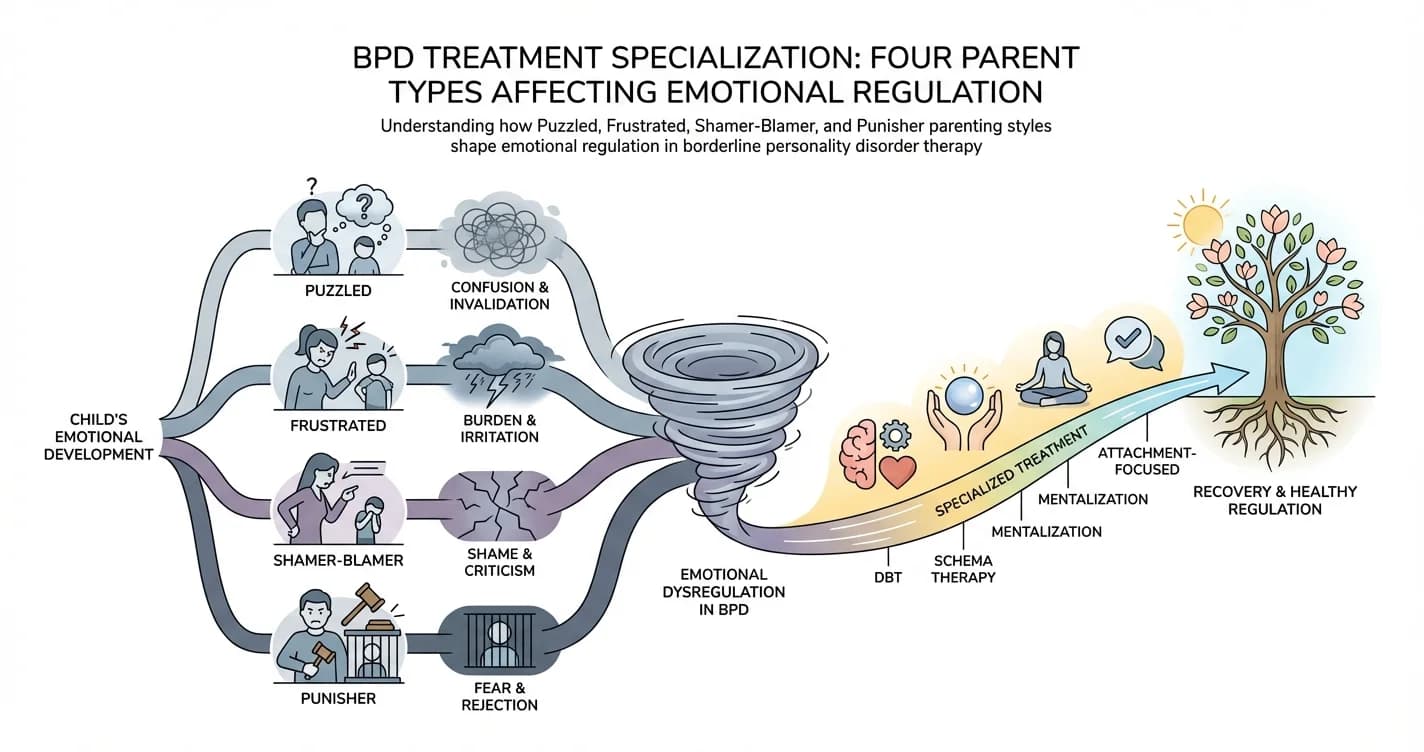
BPD Treatment Specialization: Four Parent Types Affecting Emotional Regulation
For individuals with borderline personality disorder (BPD), emotional regulation difficulties rarely emerge in isolation. Research increasingly suggests that
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
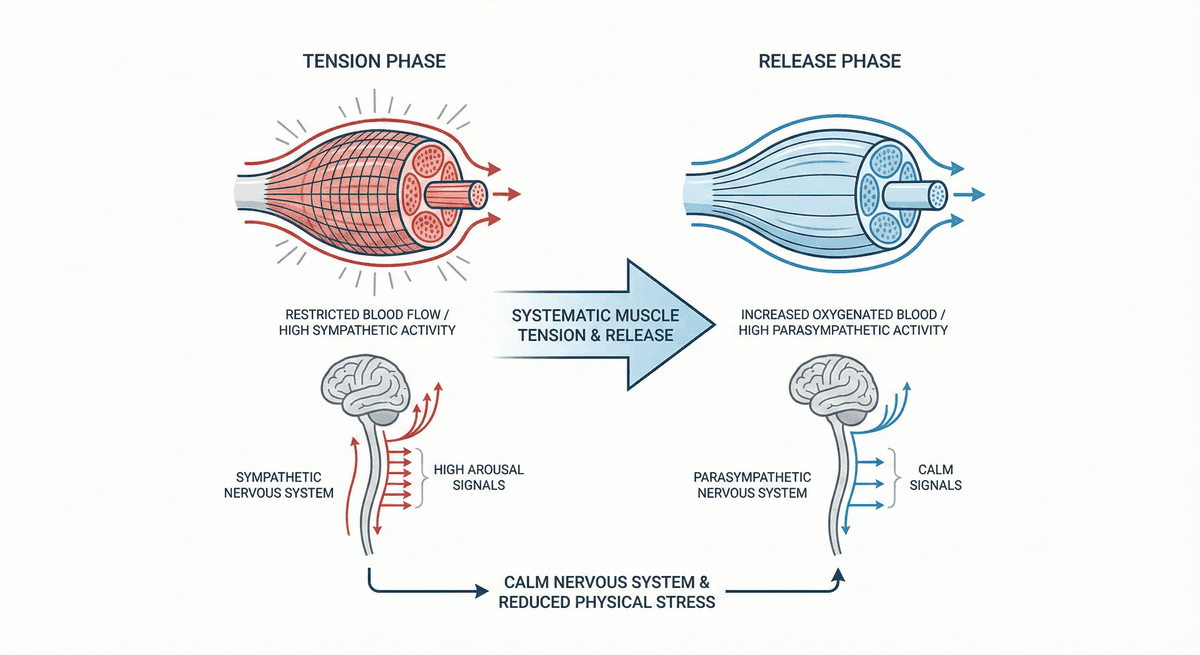
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.