Bipolar 1 vs Bipolar 2 vs Cyclothymia: 2026 Guide
Bipolar 1 means full mania; bipolar 2 means hypomania plus depression; cyclothymia means chronic sub-threshold cycling. See exactly what sets them apart in 2026.
Key Takeaways
- A basic understanding that "bipolar" is a spectrum, not a single condition
- Awareness that diagnosis requires a licensed clinician — this article is educational, not diagnostic
- Time: roughly 10 minutes to read through the full breakdown
- A mood tracking app or journal if you want to bring symptom patterns to a clinical appointment
- At least one manic episode lasting 7 or more days, or severe enough to require hospitalization or emergency intervention
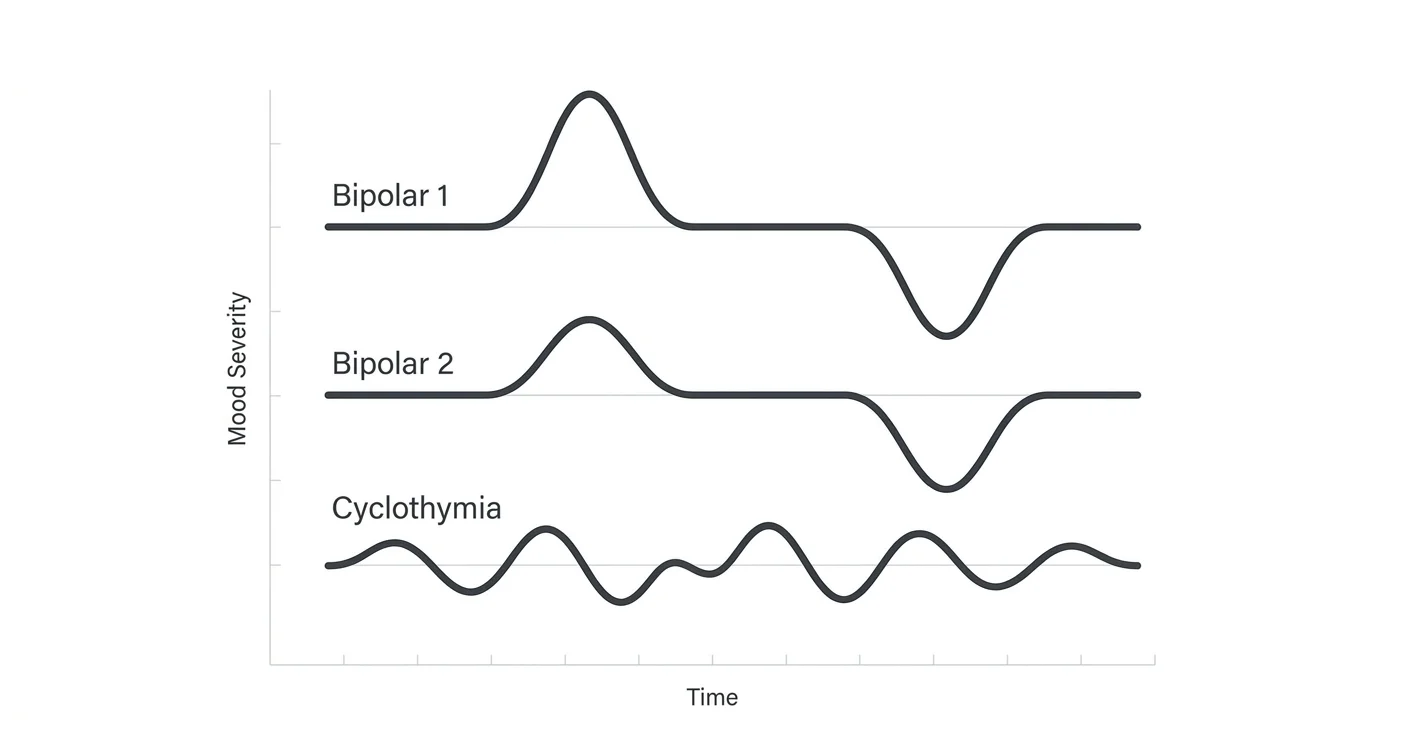
The three bipolar spectrum disorders — bipolar 1, bipolar 2, and cyclothymia — share mood cycling as a common thread, but they differ sharply in severity, episode type, and what daily life actually looks like. Knowing which is which matters because the wrong diagnosis leads to the wrong treatment.
TL;DR: Bipolar 1 involves full manic episodes lasting at least 7 days that often require hospitalization; bipolar 2 involves hypomania (a milder high) plus major depression; cyclothymia involves chronic low-grade mood swings for at least 2 years that never fully meet criteria for mania or major depression. In 2026, all three are distinct DSM-5 diagnoses with different treatment protocols. If you recognize these patterns in yourself, a licensed clinician is the right next step — not self-diagnosis.
Why the distinction matters
Many people search "bipolar 1 vs bipolar 2 vs cyclothymia" because they've been told they have mood swings but aren't sure which label fits — or they've received conflicting diagnoses. The stakes are real. Certain antidepressants used without a mood stabilizer can trigger a manic episode in someone with bipolar 1. Cyclothymia is frequently dismissed as "just being moody," which means people miss targeted support for years. Getting the right frame changes what you do next.
What you'll need before reading further
- A basic understanding that "bipolar" is a spectrum, not a single condition
- Awareness that diagnosis requires a licensed clinician — this article is educational, not diagnostic
- Time: roughly 10 minutes to read through the full breakdown
- A mood tracking app or journal if you want to bring symptom patterns to a clinical appointment
Step 1: Understand the core building blocks — mood episode types
Every bipolar spectrum diagnosis is built from the same raw materials: specific types of mood episodes. Before comparing the three disorders, you need to know what each episode type actually means.
Mania is a distinct period of abnormally elevated, expansive, or irritable mood plus increased energy lasting at least 7 days (or any duration if hospitalization is required). During a manic episode a person typically needs little sleep, talks fast, has racing thoughts, and may engage in reckless behavior — spending, risky sex, impulsive business decisions. Mania is severe enough to cause marked impairment in social or occupational functioning.
Hypomania looks like mania's quieter sibling. The same elevated mood and energy are present, but the episode lasts at least 4 consecutive days, is noticeable to others, and represents a clear change from baseline — yet it does not cause severe impairment and does not require hospitalization. Many people in a hypomanic episode feel highly productive and don't recognize it as a symptom until they crash.
Major depressive episodes last at least 2 weeks and include 5 or more symptoms such as depressed mood, loss of interest, sleep disruption, fatigue, difficulty concentrating, feelings of worthlessness, or thoughts of death. This is the same depression criteria used for major depressive disorder.
Hypomanic/depressive symptoms in cyclothymia never fully meet the criteria for a hypomanic episode or a major depressive episode — they are sub-threshold on both ends.
Step 2: Map bipolar 1 — the full mania diagnosis
Bipolar 1 is defined by the presence of at least one lifetime manic episode. That's it. A major depressive episode is common but not required for the diagnosis.
Key markers in 2026 clinical criteria:
- At least one manic episode lasting 7 or more days, or severe enough to require hospitalization or emergency intervention
- The manic episode is not better explained by substance use or another medical condition
- Most people with bipolar 1 also experience depressive episodes, but the manic episode alone qualifies
What this feels like day-to-day: During a manic phase a person may go 3 or 4 nights with almost no sleep and feel fine — even energized. Thoughts come faster than they can speak them. Grandiosity is common: the belief that one has special abilities or connections. After the manic episode ends, there is often a depressive crash that can last weeks or months. Between episodes, many people with bipolar 1 function at a high level, which is why the disorder is sometimes missed for years.
Treatment typically involves: Mood stabilizers (lithium is the best-studied), atypical antipsychotics during acute mania, and ongoing psychiatric care. Antidepressants used alone are generally avoided.
Step 3: Map bipolar 2 — hypomania plus significant depression
Bipolar 2 requires at least one hypomanic episode and at least one major depressive episode. Crucially, there has never been a full manic episode — if mania appears at any point, the diagnosis upgrades to bipolar 1.
Key markers:
- Hypomania: elevated or irritable mood for at least 4 consecutive days, observable by others, but not causing severe impairment
- At least one major depressive episode (5+ symptoms for 2+ weeks)
- No history of a full manic episode
What this feels like day-to-day: Hypomanic phases often feel like "finally being yourself" — sharper, more social, more productive. Because hypomania doesn't feel like a problem, people with bipolar 2 often present to clinicians only during depressive episodes, which is why bipolar 2 is frequently misdiagnosed as major depression for years before the hypomanic pattern is identified. The depressive episodes in bipolar 2 tend to be longer and more frequent than in bipolar 1, making depression the dominant burden for most people with this diagnosis.
Treatment typically involves: Mood stabilizers or atypical antipsychotics, psychotherapy (especially CBT and interpersonal social rhythm therapy), and careful monitoring of antidepressant use.
Step 4: Map cyclothymia — chronic sub-threshold mood cycling
Cyclothymia is a chronic mood disorder characterized by numerous periods of hypomanic symptoms and depressive symptoms over at least 2 years (1 year in adolescents), without ever meeting full criteria for a hypomanic episode or a major depressive episode. During those 2 years, the person has not been symptom-free for more than 2 consecutive months.
Key markers:
- Sub-threshold hypomania: elevated mood and energy that don't quite hit the 4-day minimum or full symptom count for hypomania
- Sub-threshold depression: low mood, low energy, reduced pleasure that don't quite reach 5 symptoms for 2 weeks
- Chronic pattern: symptoms present for at least 2 years
- Approximately 15–50% of people with cyclothymia go on to develop bipolar 1 or bipolar 2, according to DSM-5 estimates
What this feels like day-to-day: Life feels unpredictable. Good days cluster, then bad weeks arrive without obvious cause. Relationships are strained because others can't predict mood state. Because neither the highs nor the lows are severe enough to trigger obvious crises, cyclothymia often goes undiagnosed for a decade or more. People are frequently told they're "sensitive" or "temperamental" rather than receiving targeted support.
Treatment typically involves: Mood stabilizers, CBT focused on behavioral activation and sleep regulation, and lifestyle structure. The same 2-year threshold that defines the diagnosis also means early intervention can potentially prevent progression to a full bipolar diagnosis.
Step 5: Use a side-by-side comparison to lock in the differences
| Feature | Bipolar 1 | Bipolar 2 | Cyclothymia |
|---|---|---|---|
| Defining episode | Full mania (7+ days) | Hypomania + major depression | Sub-threshold both ends |
| Hospitalization risk | High during mania | Low | Very low |
| Depression present | Common, not required | Required for diagnosis | Sub-threshold, always present |
| Duration criteria | 7 days for mania | 4 days for hypomania; 2 weeks for depression | 2 years of cycling |
| Functional impairment | Severe during mania | Moderate (mostly from depression) | Mild to moderate, chronic |
| Misdiagnosis risk | Sometimes called psychosis | Frequently called MDD | Frequently dismissed entirely |
| Progression risk | Stable diagnosis | ~5–15% convert to bipolar 1 | 15–50% may develop bipolar 1 or 2 |
Step 6: Recognize what all three share — and where the overlap creates confusion
All three disorders involve:
- Cycling between elevated and depressed mood states
- Sleep disruption as both a trigger and a symptom
- Impaired relationships and work performance during active phases
- A need for ongoing management, not just acute treatment
The overlap creates real diagnostic confusion. Someone in a mild hypomanic episode who only seeks help during depression will look like they have major depressive disorder. Someone with cyclothymia who has a particularly bad stretch may look like bipolar 2. This is why longitudinal mood tracking — writing down mood, sleep, energy, and behavior daily for several months — is one of the most useful things a person can bring to a psychiatric evaluation in 2026.
Troubleshooting: common points of confusion
"I have bipolar 2 but my psychiatrist mentioned bipolar 1 — is that a mistake?" Not necessarily. If a full manic episode occurred at any point — including one that happened years ago and wasn't recognized as mania at the time — the diagnosis shifts to bipolar 1. A thorough history review sometimes uncovers this.
"My therapist said cyclothymia isn't a real diagnosis." Cyclothymia is a formal DSM-5 and ICD-11 diagnosis. It is less studied than bipolar 1 and 2, but it is real, it is treatable, and dismissing it delays support.
"I feel fine between episodes — does that mean I don't have bipolar?" Interval wellness is common, especially in bipolar 1. Feeling fine between episodes does not rule out the diagnosis. It also doesn't mean treatment should stop during those intervals.
"Can you have bipolar and anxiety at the same time?" Yes. Comorbid anxiety disorders — generalized anxiety, social anxiety, panic disorder — are present in more than 50% of people with bipolar spectrum diagnoses, based on large-scale epidemiological studies. Treating only one without addressing the other limits outcomes.
"How long does it usually take to get the right diagnosis?" Studies published before 2026 consistently show an average delay of 6–10 years between first symptoms and correct bipolar diagnosis. Tracking mood patterns and being specific with a clinician about the timing and nature of high-energy periods shortens that gap.
"Is bipolar 2 less serious than bipolar 1?" Not in terms of life impact. Bipolar 2 carries a high burden of depression, and the suicide risk is comparable to bipolar 1. "Less severe" refers only to the absence of full mania — not to quality of life or the need for treatment.
Tools and resources
- Mood tracking apps or a paper journal: Daily logging of mood (1–10 scale), sleep hours, energy, and notable events is the most actionable tool before a clinical appointment.
- A licensed psychiatrist: Bipolar spectrum diagnoses require a clinical evaluation — not a self-assessment quiz. A GP can provide a referral.
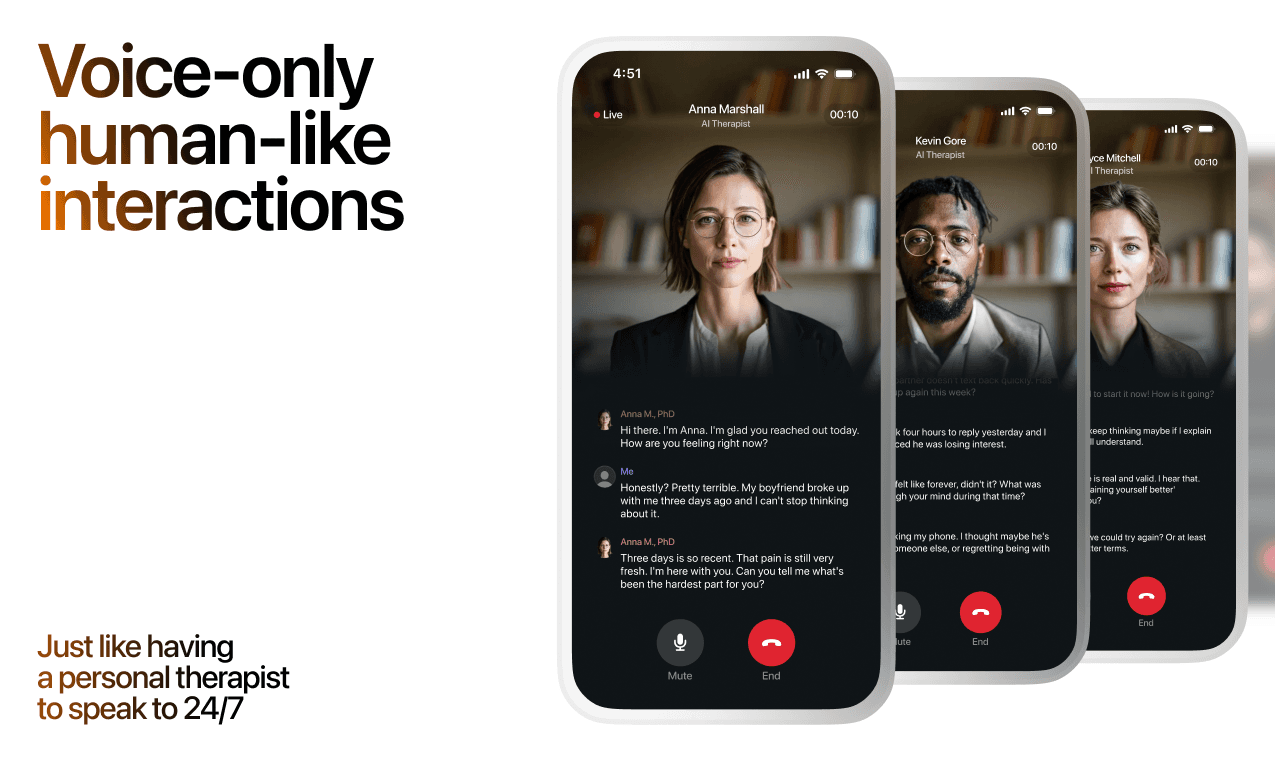
- Lovon: If you're waiting for a clinical appointment or managing day-to-day emotional strain, Lovon's AI voice therapy app gives you a space to talk through what you're feeling, build coping habits, and process stress. It is not a substitute for psychiatric care, but it can help with the emotional weight between sessions. See what free AI therapy for depression support looks like, or explore AI therapy for anxiety and panic attacks — both common co-occurring concerns in bipolar spectrum disorders.
- NAMI (National Alliance on Mental Illness): Free peer-support programs, including group programs specifically for mood disorders.
FAQ
What is the main difference between bipolar 1 and bipolar 2? Bipolar 1 requires at least one full manic episode lasting 7 or more days severe enough to cause significant impairment. Bipolar 2 requires hypomania — a milder, shorter elevated mood lasting at least 4 days — plus at least one major depressive episode, and no history of full mania.
Is cyclothymia the same as bipolar disorder? Cyclothymia is on the bipolar spectrum but is a distinct diagnosis. It involves 2 or more years of sub-threshold mood swings that never fully meet criteria for hypomania or major depression. Roughly 15–50% of people with cyclothymia go on to develop bipolar 1 or bipolar 2.
Can bipolar 2 turn into bipolar 1? Yes. If a person with a bipolar 2 diagnosis experiences a full manic episode, the diagnosis changes to bipolar 1. Studies estimate this conversion happens in approximately 5–15% of people with bipolar 2.
How is cyclothymia diagnosed? A clinician looks for at least 2 years of alternating hypomanic-like and depressive-like symptoms that never meet the full threshold for either hypomania or a major depressive episode, with no symptom-free stretch longer than 2 months.
What triggers mania in bipolar 1? Sleep deprivation is one of the most consistent triggers across research literature. Other common triggers include major life stress, stimulant use, and starting certain antidepressants without a mood stabilizer.
Can you have bipolar disorder and not know it? Yes, and it is common. The average time between first symptoms and correct diagnosis is 6–10 years. Bipolar 2 is especially likely to be missed because hypomania often feels positive rather than disruptive, so people only seek help during depressive episodes.
What is the best treatment for bipolar spectrum disorders in 2026? Treatment is always individualized. Mood stabilizers (lithium, valproate, lamotrigine) and certain atypical antipsychotics are first-line pharmacological options. Psychotherapy — particularly CBT and interpersonal social rhythm therapy — is strongly evidence-supported alongside medication.
Is it possible to live well with bipolar disorder? Yes. With the right combination of medication, therapy, sleep regulation, and support, the majority of people with bipolar spectrum diagnoses maintain stable employment, relationships, and quality of life. Early and accurate diagnosis is the biggest predictor of long-term outcome.
One last thing
Cyclothymia carries an often-overlooked risk: because neither the highs nor the lows ever feel severe enough to be a "real" problem, people spend years assuming they're just wired that way. But those 2 years of sub-threshold cycling are doing real damage to sleep, relationships, and career stability — even without a dramatic crisis. If the cyclothymia pattern sounds familiar, the absence of dramatic episodes is not evidence that nothing is wrong.
Related guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
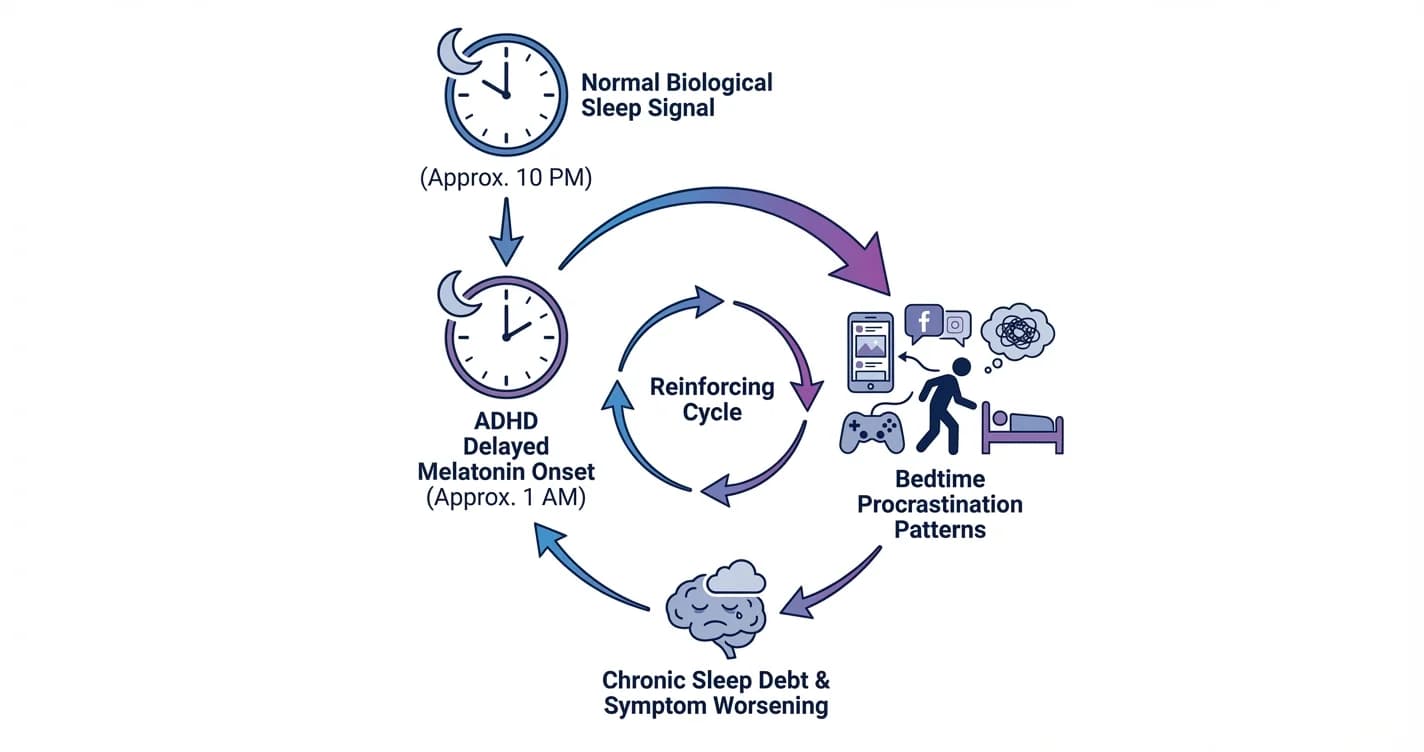
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
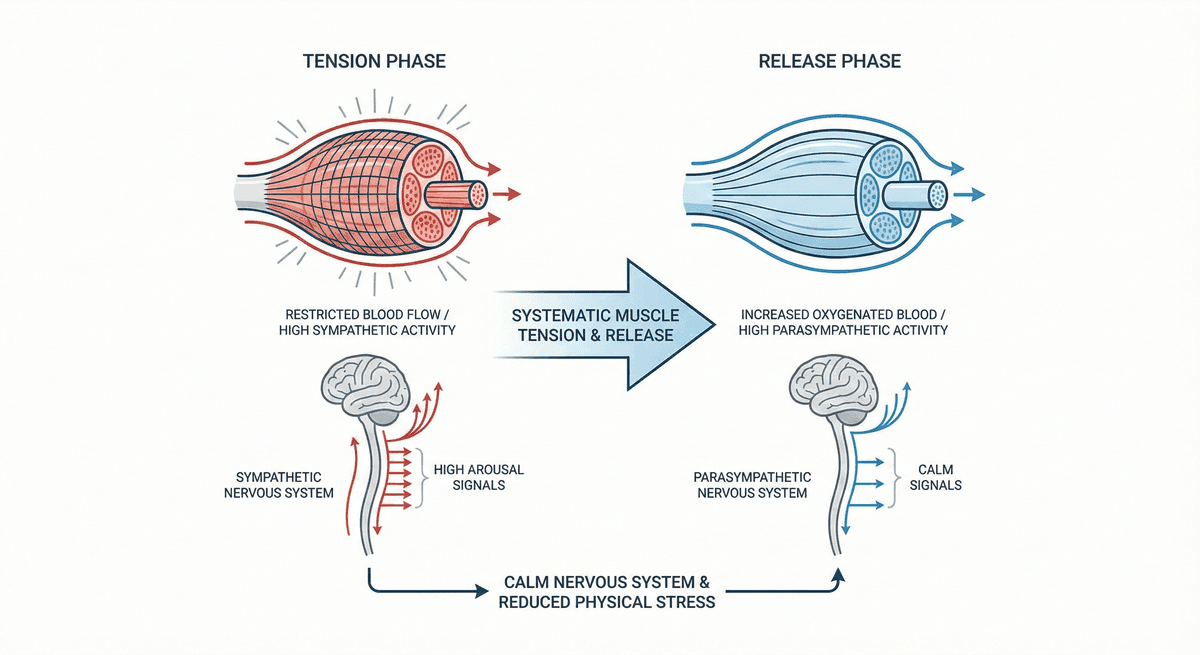
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.