BPD Attachment Style: The Push-Pull Cycle Explained 2026
BPD attachment style is almost always disorganized. Learn what drives the push-pull cycle, the 5-step loop, and what actually changes it in 2026.
Key Takeaways
- A basic understanding that attachment styles form in childhood based on caregiver responses
- Willingness to hold two truths at once: BPD behavior can be painful to be around and it comes from genuine suffering
- No prior clinical knowledge required — plain language throughout
- Time: roughly 10 minutes to read fully
- DBT workbooks — skills like TIPP (Temperature, Intense exercise, Paced breathing, Progressive muscle relaxation)
BPD attachment style sits at the center of some of the most confusing relationship dynamics a person can experience — the intense pull toward closeness followed by a sudden push toward distance, cycling back again before either person can catch their breath.
TL;DR: The BPD attachment style is almost always disorganized — meaning the same person who feels like safety also feels like a threat. This creates the push-pull cycle: desperate closeness, then withdrawal, then panic, then closeness again. It is driven by fear of abandonment, an unstable sense of self, and a nervous system that reads neutral cues as danger. In 2026, attachment research increasingly links BPD to early relational trauma, not a character flaw. Understanding the mechanics gives you — or someone you love — a real starting point for change.
Why this matters
BPD affects roughly 1.6% of the general population, but that number rises to about 20% among psychiatric inpatients. The push-pull behavior it produces does not happen because someone is manipulative or selfish. It happens because their attachment system is wired to treat intimacy and danger as the same signal. When you understand that, the pattern stops looking irrational and starts looking like a very logical response to a very early wound.
What you'll need before you read on
- A basic understanding that attachment styles form in childhood based on caregiver responses
- Willingness to hold two truths at once: BPD behavior can be painful to be around and it comes from genuine suffering
- No prior clinical knowledge required — plain language throughout
- Time: roughly 10 minutes to read fully
The four attachment styles and where BPD lands
Attachment theory identifies four main styles: secure, anxious, avoidant, and disorganized (also called fearful-avoidant). People with BPD almost never land in the secure category. Research published across multiple studies consistently places BPD attachment style in the disorganized or anxious range — often both at different points in the same relationship.
Disorganized attachment is the one where the attachment figure was also the source of fear. A child whose caregiver was unpredictable, frightening, or abusive learns a brutal lesson: the person I need to survive is the person I cannot trust. That conflict does not resolve — it goes underground and resurfaces in every close relationship in adulthood.
Anxious attachment in BPD
The anxious piece shows up as hypervigilance to rejection cues. A slow text reply reads as abandonment. A neutral tone of voice reads as anger. A partner needing alone time reads as "they are leaving me." The nervous system fires as if the threat is real, because emotionally it is real — the brain is pattern-matching to early experiences where that slow reply or that neutral tone actually did mean abandonment.
Disorganized attachment in BPD
This is the layer that produces the push-pull directly. The person with BPD craves closeness and simultaneously fears it. When a partner gets too close, the old threat signal fires — intimacy is dangerous — and they pull back, sometimes with sudden coldness or manufactured conflict. When the partner responds by withdrawing, the abandonment fear fires — I am being left — and they pull the partner back in. Neither state lasts. Neither state feels chosen.
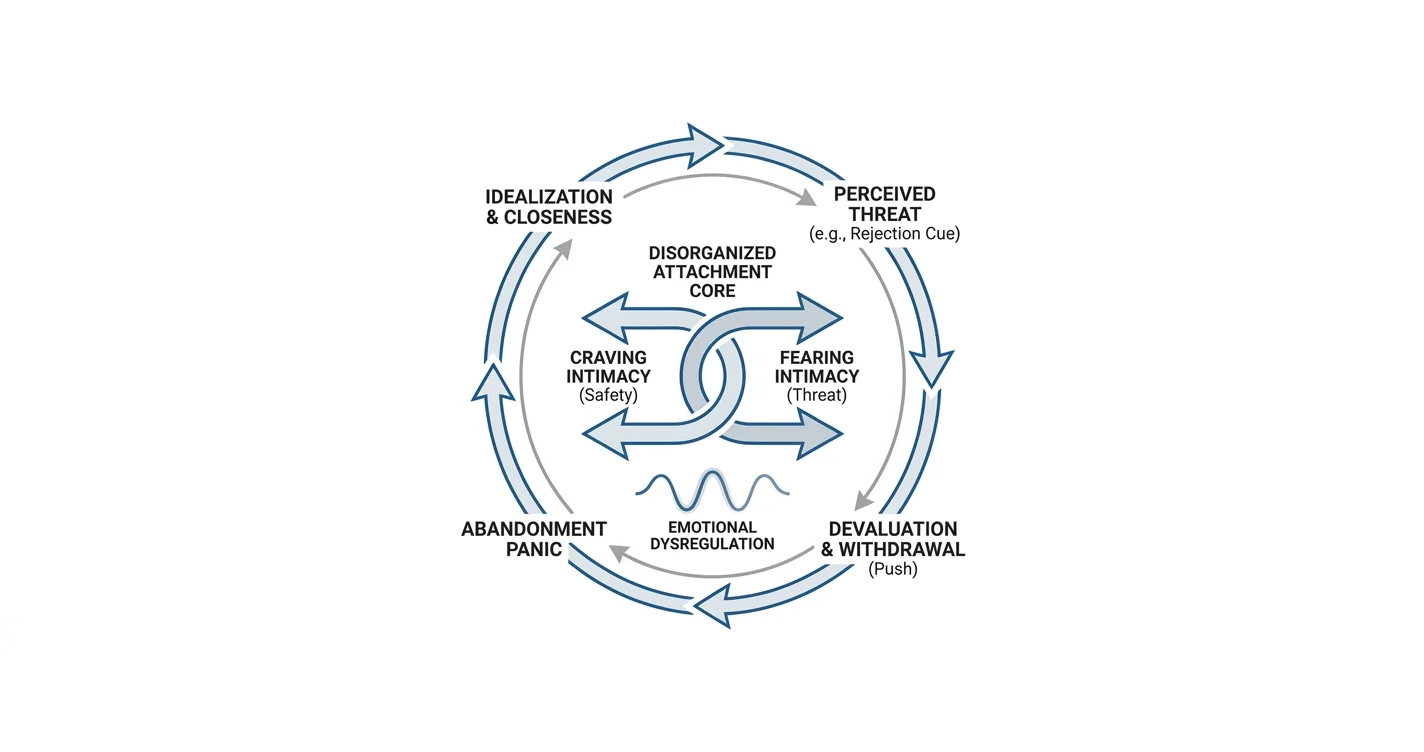
The push-pull cycle: how it actually works, step by step
Step 1 — Idealization fires first
A new relationship or a repaired rupture triggers a flood of positive attachment. The person with BPD experiences the other person as perfect, safe, and the answer to a deep loneliness. This is not performance — it is a genuine neurological state. Dopamine and attachment hormones spike hard. Everything feels urgent and real.
Common mistake: Partners interpret this intensity as deep love and match it, which sets the baseline impossibly high for what comes next.
Step 2 — The threat signal activates
Something — often minor from the outside — trips the disorganized attachment wire. A cancelled plan. A shift in tone. Perceived criticism. The brain registers this as the early wound repeating. Cortisol rises. The amygdala treats the situation as an emergency. Emotional regulation, which is already harder in BPD due to differences in prefrontal-limbic connectivity, drops further. For a deeper look at how this brain process works, the amygdala hijack article explains the neuroscience clearly.
Expected outcome of this step: Rapid mood shift — from warm to cold, from open to hostile, from pulled-in to pushing away.
Step 3 — Devaluation and withdrawal
The person who felt perfect in Step 1 now feels dangerous or inadequate. This is the classic BPD "splitting" — the cognitive inability in a dysregulated state to hold both good and bad qualities of a person simultaneously. The partner is now all bad. The person with BPD may withdraw, pick fights, or say things designed to create distance.
What this accomplishes emotionally: Distance = safety from the threat signal. The nervous system briefly calms.
Step 4 — Abandonment panic sets in
The distance that felt protective now triggers the other terror: being left. Within hours, days, or weeks, the fear of abandonment overrides the fear of closeness. Attempts at reconnection begin — apologies, affection, idealization again. The partner who was all bad is now all good again.
Common mistake: Both people interpret the reconnection as the problem being solved. It is not solved — the cycle has just reset to Step 1.
Step 5 — The cycle repeats
Without intervention, the loop runs indefinitely. Each cycle tends to escalate — higher highs, lower lows, faster transitions. Partners often describe feeling like they are "walking on eggshells" even during the good phases, because they have learned the shift is coming.
What drives it at the root: three core mechanisms
1. Emotional dysregulation. The BPD nervous system reacts faster and more intensely than average, and it takes longer to return to baseline. A 2019 meta-analysis covering 48 studies found that emotional dysregulation is present in 93% of BPD cases. The push-pull is partly just the attachment system riding those emotional swings.
2. Identity instability. Without a stable sense of self, relationships become mirrors. The person with BPD looks to their partner to confirm who they are. When the partner is "good," the self feels coherent. When the partner disappoints, the self collapses — which is intolerable, so the partner becomes the problem.
3. Early relational trauma. In 2026, the clinical consensus has moved firmly toward viewing BPD as a trauma-spectrum condition in most cases. Childhood environments characterized by emotional invalidation, unpredictable caregiving, or abuse produce exactly the disorganized attachment pattern that defines the BPD attachment style. The father wound vs mother wound article goes deeper on how specific early relational dynamics shape adult patterns.
Troubleshooting: when the cycle looks different
"My partner with BPD doesn't idealize me — they just seem angry." Idealization is not always visible to the partner. It can present as possessiveness, intense jealousy, or anxiety about losing you rather than overt praise. The underlying attachment drive is the same.
"I have BPD and I freeze instead of pushing away." Some people with BPD move into a freeze or shutdown state rather than overt conflict. This is still the same disorganized attachment pattern — the threat response just routes through immobilization rather than anger. The freeze response article covers why this happens and what it feels like from inside.
"We've done therapy and the cycle still happens." Dialectical Behavior Therapy (DBT) is the gold-standard treatment for BPD, with the strongest evidence base. Progress is real but non-linear. A return of the cycle after a calm period does not mean treatment failed — it means the nervous system encountered a sufficiently strong trigger. Continued practice of distress tolerance and interpersonal effectiveness skills from DBT is the appropriate response, not stopping therapy.
"My partner accuses me of causing the cycle." Partners of people with BPD can develop their own anxious or avoidant patterns in response to the cycling, which then become genuine triggers. This is not blame — it is feedback. Couples therapy alongside individual DBT addresses this most effectively.
"How do I know if this is BPD or anxious attachment without BPD?" Intensity and breadth of symptoms. Anxious attachment alone produces hypervigilance and clinginess but does not typically include identity instability, self-harm, or the rapid full-switch from idealization to devaluation. A formal clinical assessment from a licensed therapist is the only reliable way to differentiate.
"Does this ever actually change?" Yes. A landmark 10-year follow-up study found that 85% of people with BPD achieved remission of symptoms over that period. Change is possible — it requires consistent work and usually professional support, but the prognosis is far better than most people believe in 2026.
Tools and resources
- DBT workbooks — skills like TIPP (Temperature, Intense exercise, Paced breathing, Progressive muscle relaxation) directly address the emotional dysregulation that drives the cycle
- NAMI (National Alliance on Mental Illness) — free educational resources and peer support groups for people with BPD and their partners
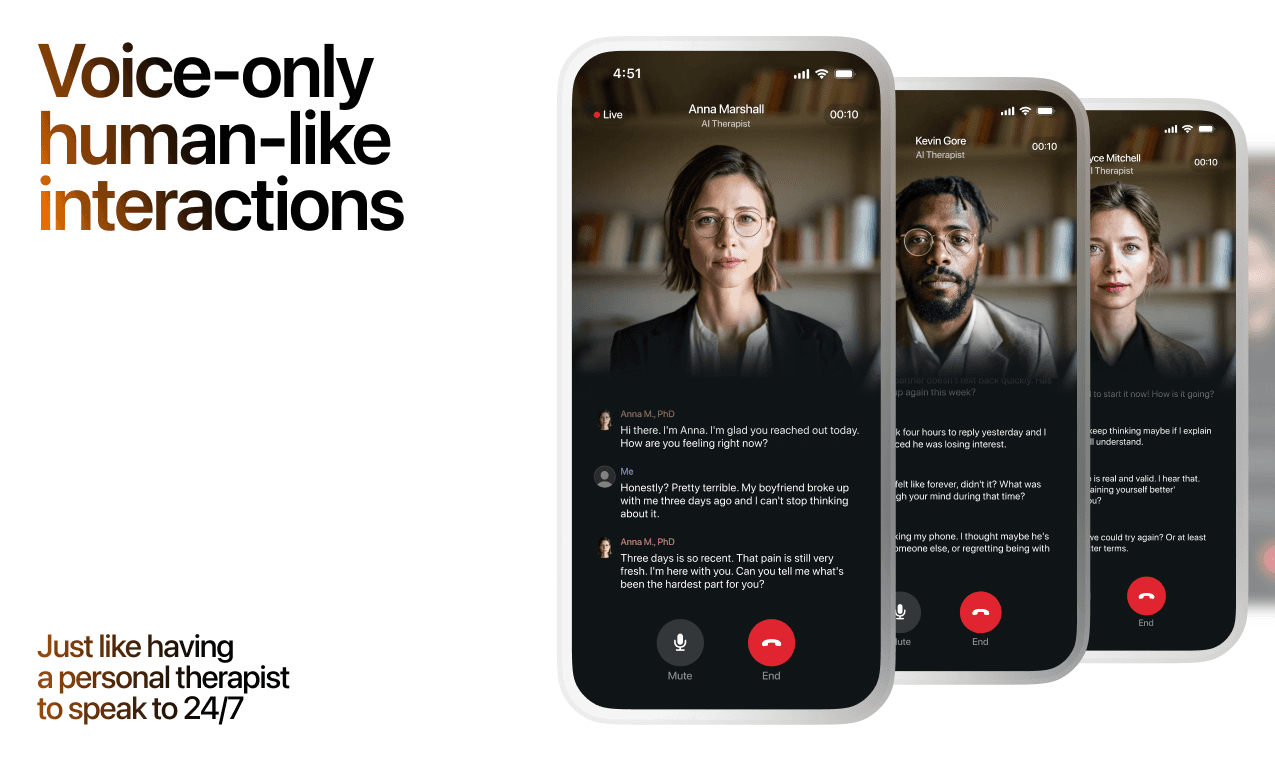
- Lovon — the Lovon app offers on-demand voice conversations with an AI therapist for moments when the emotional intensity spikes and a human therapist isn't immediately available. It is not a substitute for DBT or licensed clinical care, but it gives you a real-time place to process before you act on an impulse
- For relationship-specific patterns that often co-occur with BPD dynamics, the pursuer-withdrawer pattern article is directly relevant
What to do next
If you recognized the push-pull cycle in your own relationships — whether you are the person with BPD or the partner — the single most important next step is a formal assessment with a therapist who specializes in personality disorders. Understanding the BPD attachment style conceptually is useful. Having a professional map your specific pattern and match it to evidence-based tools is what actually moves the needle.
In 2026, DBT is available in individual, group, and app-based formats. Access is better than it has ever been.
FAQ
What is the BPD attachment style? The BPD attachment style is almost always disorganized or fearful-avoidant, meaning the person simultaneously craves closeness and fears it. This produces the push-pull dynamic — cycling between idealization and devaluation — because both intimacy and distance trigger their own distinct fear responses.
Is BPD the same as anxious attachment? No. Anxious attachment is a dimension of the BPD attachment style, but BPD includes identity instability, more extreme emotional swings, and the specific splitting behavior — seeing people as all-good or all-bad — that anxious attachment alone does not produce.
Can someone with BPD have a stable relationship in 2026? Yes. With consistent DBT treatment and a partner who understands the attachment dynamics, stable long-term relationships are achievable. Research from multi-year follow-up studies shows significant symptom reduction over time for most people who engage with treatment.
What triggers the push in the push-pull cycle? Usually a perceived threat to the relationship — a cancelled plan, a change in tone, criticism, or a partner spending time away. The trigger does not have to be objectively significant; what matters is how the dysregulated nervous system reads it against the background of early relational experience.
How do you support a partner with BPD without losing yourself? Clear, consistent boundaries stated calmly — not punitively. Your own therapy, separate from couples work. Learning to distinguish between responding to real distress and reinforcing the cycle. You cannot stabilize the attachment system of another person; you can only make your own responses predictable, which reduces one source of triggering.
What's the best therapy for BPD attachment patterns? DBT is the most evidence-supported treatment for BPD specifically. Schema Therapy and Mentalization-Based Treatment (MBT) also show strong results, particularly for the attachment and identity components. No single approach works for everyone — treatment matching matters.
Is the push-pull cycle in BPD intentional? No. People with BPD are not consciously running a manipulation script. The cycle is driven by automatic threat responses in a dysregulated nervous system. That does not make the behavior painless for partners, but it does mean the path forward is skills-based intervention, not blame.
How long does it take to change BPD attachment patterns? DBT programs typically run 6 to 12 months for the structured skills component. Actual change in attachment patterns takes longer — often 2 to 4 years of consistent work. The 85% remission rate in 10-year studies shows the trajectory is real, but it is not fast.
One last thing
The push-pull cycle in BPD is not a sign that the person doesn't want a real connection. It is a sign that real connection feels like the most dangerous thing in the world to a nervous system shaped by early relational pain. In 2026, that is treatable. The first step is naming it accurately — which you just did.
Related guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
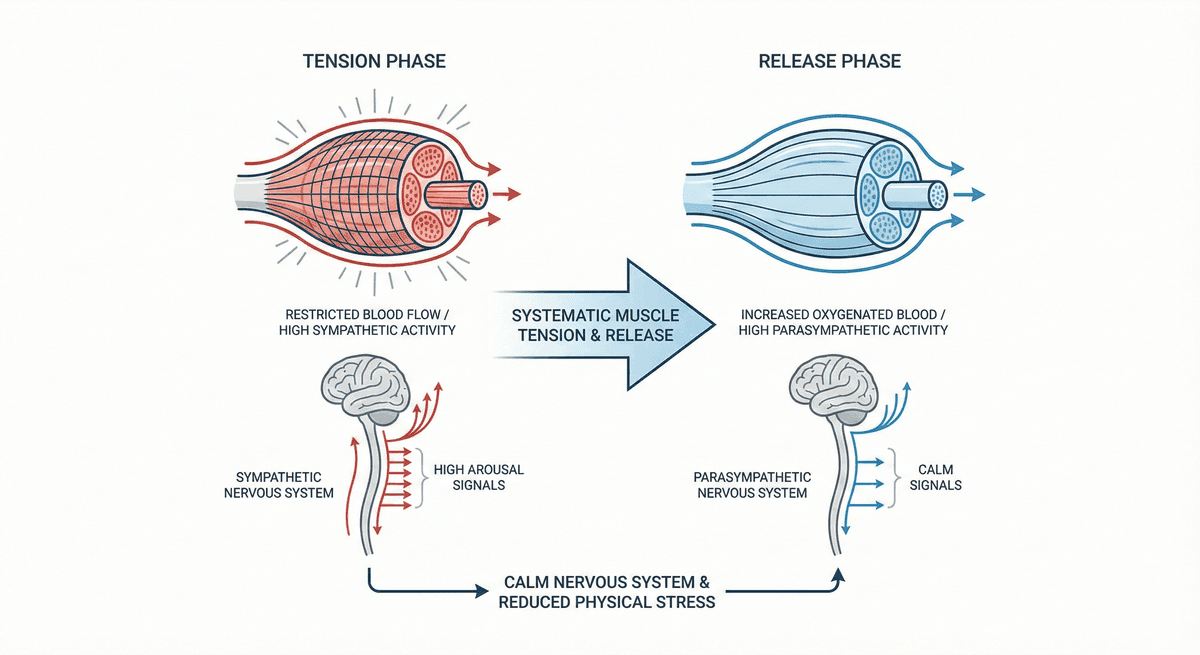
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
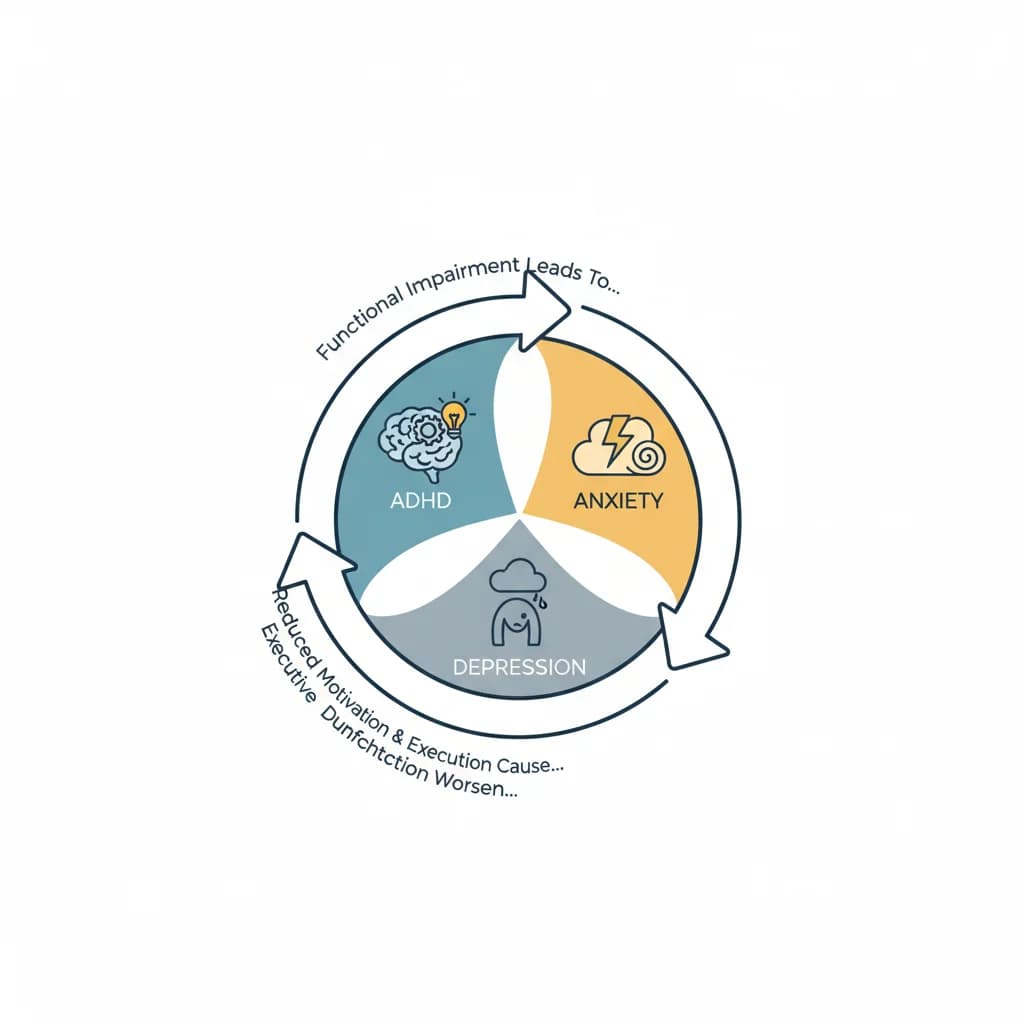
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
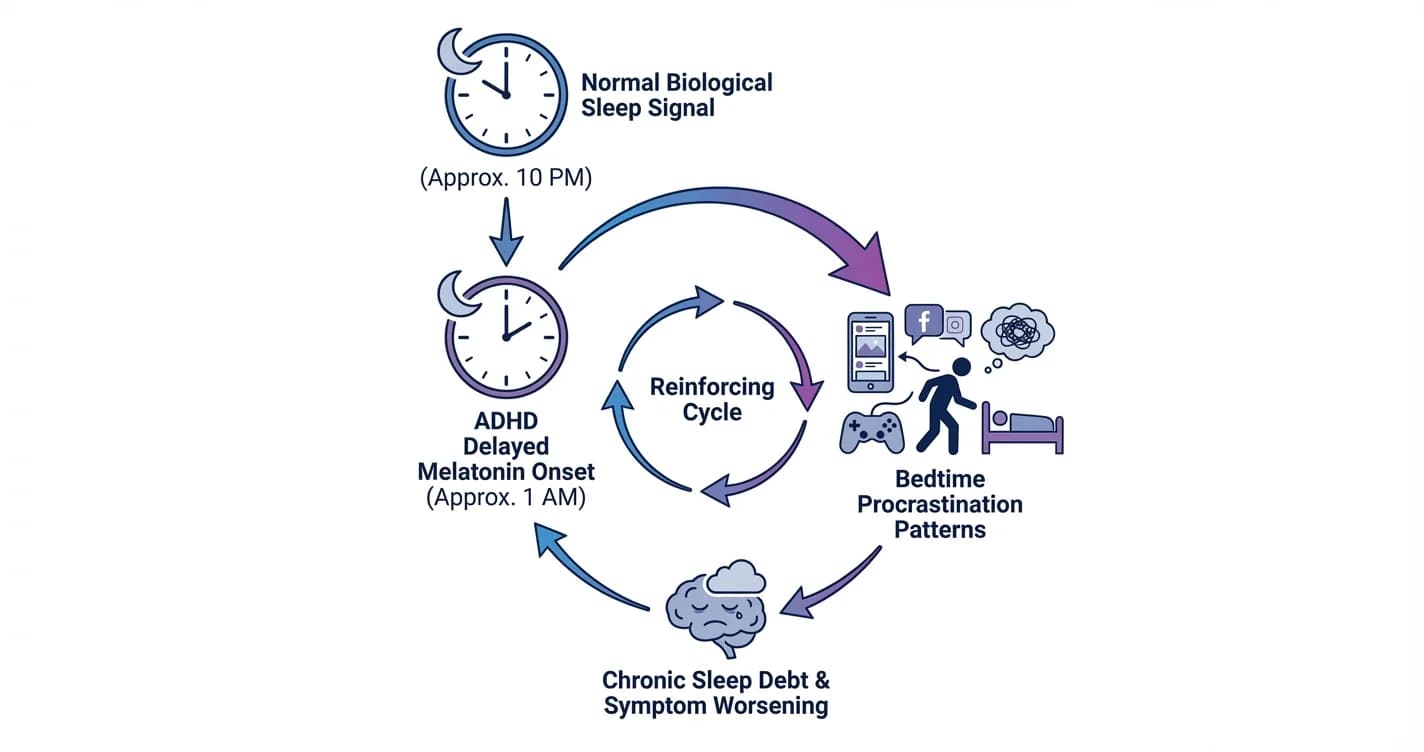
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.