Complex PTSD vs PTSD: What Sets Them Apart (2026)
Complex ptsd vs ptsd explained: trauma origin, symptom clusters, and self-assessment steps. See the 2026 diagnostic differences and what to do next.
Key Takeaways
- A rough timeline of your trauma history — one event, or repeated/prolonged exposure
- A current symptom list (write it down, don't rely on memory alone)
- 15-20 minutes of quiet time for honest self-reflection
- Access to a licensed mental health professional for actual diagnosis (self-assessment is a starting point, not a
- Optional: a [polyvagal theory primer](https://lovon.app/blog/mental-health/polyvagal-theory-explained-stress-safety-a...
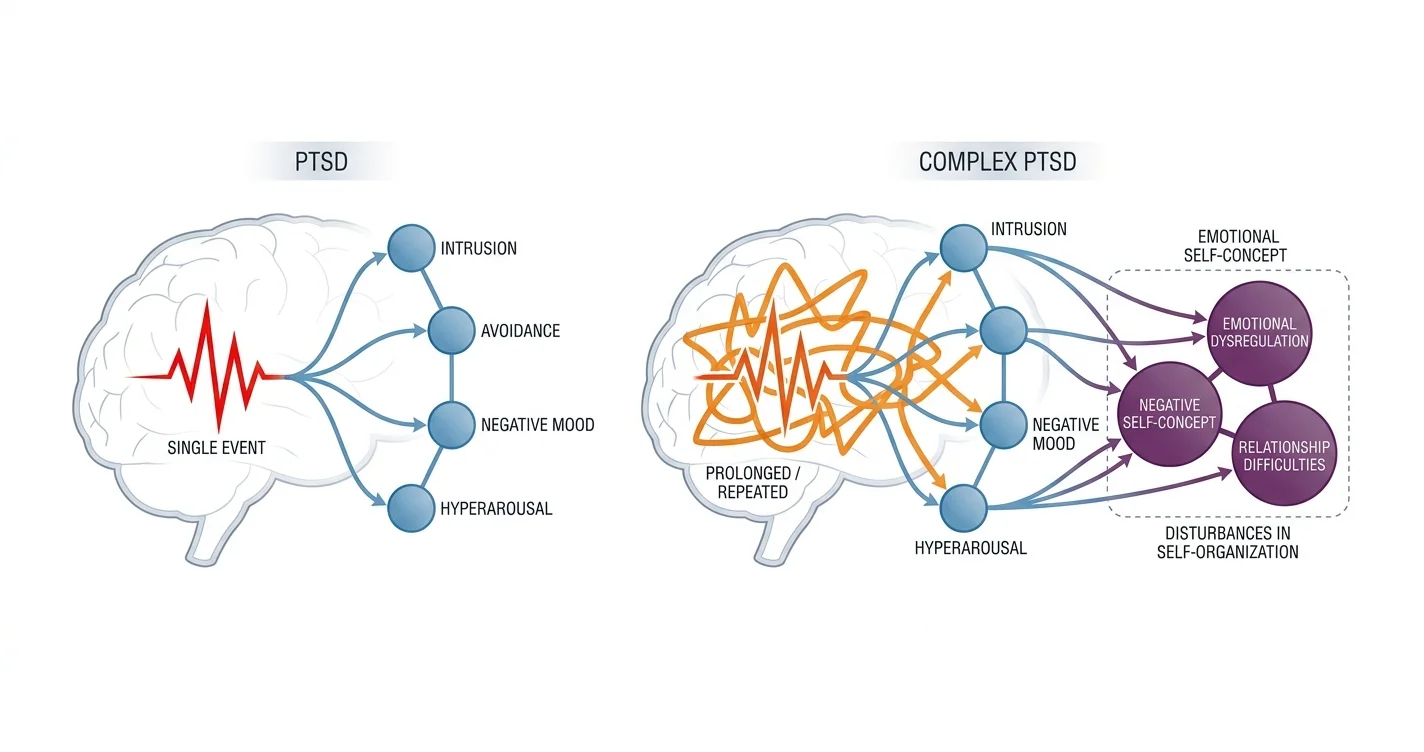
Complex PTSD and PTSD share a root cause — trauma — but they don't look the same on the inside, and mixing them up can send you toward the wrong kind of help for years.
TL;DR: Complex PTSD (CPTSD) develops from prolonged or repeated trauma — childhood abuse, captivity, ongoing domestic violence — and adds three symptoms on top of standard PTSD: emotional dysregulation, a persistently negative self-view, and relationship difficulties. PTSD typically follows a single traumatic event — an accident, an assault, a disaster — and centers on intrusion, avoidance, negative mood changes, and hyperarousal. In the complex ptsd vs ptsd comparison, the practical difference is duration and origin: one event versus a pattern. Verdict: if your symptoms trace back to years of chronic harm rather than one incident, CPTSD screening tools fit your experience better than a standard PTSD checklist, and a licensed clinician should confirm either diagnosis in 2026.
Why this matters
A misdiagnosis costs time. Someone with CPTSD who only gets treated for standard PTSD symptoms often improves on intrusive memories but stays stuck on shame, emotional flooding, and unstable relationships — because nobody addressed the self-organization symptoms ICD-11 added when it formally recognized CPTSD in 2019.
The reverse happens too: people with single-incident PTSD get handed self-help content written for complex trauma survivors, and it doesn't match their actual symptom pattern. Getting the distinction right shapes which coping tools, which therapy modality, and which self-assessment steps actually apply to you.
What you'll need
- A rough timeline of your trauma history — one event, or repeated/prolonged exposure
- A current symptom list (write it down, don't rely on memory alone)
- 15-20 minutes of quiet time for honest self-reflection
- Access to a licensed mental health professional for actual diagnosis (self-assessment is a starting point, not a verdict)
- Optional: a polyvagal theory primer to understand why your nervous system reacts the way it does
The steps
1. Map your trauma timeline first
Before you look at symptoms, look at exposure. PTSD criteria in the DSM-5 assume a discrete, identifiable event — a car crash, combat exposure, an assault. CPTSD, as defined by the ICD-11, assumes trauma that was prolonged, repeated, or inescapable — years of childhood neglect, ongoing domestic abuse, trafficking, or extended captivity.
Write down whether your trauma was a single incident or a pattern lasting months to years. This one distinction does more diagnostic work than any symptom checklist. Common mistake: people assume CPTSD requires childhood trauma specifically — it doesn't; prolonged trauma at any age qualifies.
2. Check for the four core PTSD symptom clusters
Both conditions share these four clusters, so confirm they're present before going further:
- Intrusion — flashbacks, nightmares, unwanted memories
- Avoidance — steering clear of people, places, or thoughts tied to the trauma
- Negative changes in mood or cognition — detachment, guilt, distorted blame
- Hyperarousal — being easily startled, hypervigilant, or unable to sleep
The DSM-5 requires at least one symptom from the intrusion cluster, one from avoidance, two from mood/cognition, and two from arousal — seven minimum, from a pool of 20 possible symptoms. If you're below that threshold, you may be dealing with acute stress or a subclinical response rather than full PTSD. Expected outcome: you'll know if you meet the baseline trauma-response profile at all.
3. Screen for the three CPTSD-specific additions
This is where complex ptsd vs ptsd actually splits. ICD-11 adds three "disturbances in self-organization" symptoms on top of the four above:
- Emotional dysregulation — intense reactions, difficulty calming down, numbing
- Negative self-concept — persistent shame, feeling worthless or permanently damaged
- Relationship disturbances — trouble trusting others, avoiding closeness, or feeling disconnected from people
If all three of these are present alongside the standard four clusters, CPTSD fits better than PTSD alone. Common mistake: confusing negative self-concept with situational low mood — CPTSD's version is chronic and tied directly to the trauma narrative, not a passing bad week.
4. Rate symptom duration and persistence
PTSD symptoms must last more than one month to meet diagnostic criteria; CPTSD symptoms tend to be more entrenched, often years, because the trauma itself was ongoing. Score each symptom cluster on a rough 0-10 severity scale weekly for a month. Patterns that stay flat or worsen over 30 days point toward the chronic, relational profile of CPTSD rather than an acute stress reaction that fades.
5. Notice your relationship patterns specifically
People with CPTSD frequently show up in Lovon conversations describing the same loop: attract emotionally unavailable partners, struggle with trust, then either shut down or over-give to avoid abandonment. If this sounds familiar, cross-reference it against guides on attachment style patterns built specifically around childhood-origin complex trauma. Standard PTSD, by contrast, doesn't usually reshape someone's core relational template the same way — the fear tends to stay tied to trauma reminders rather than to intimacy itself.
6. Bring the pattern to a licensed clinician
Self-assessment narrows the picture; it doesn't replace a diagnosis. A licensed clinician will typically use structured tools — the PCL-5 for PTSD, the International Trauma Questionnaire (ITQ) for CPTSD — to confirm which profile matches. Book this step even if you feel confident in your self-assessment; overlapping symptoms between the two conditions are common enough that professional confirmation changes treatment planning.
7. Match support tools to the correct profile
Once you know which one you're dealing with, your daily coping toolkit should shift. CPTSD benefits heavily from nervous-system regulation work and relational-pattern awareness; standard PTSD often responds faster to trauma-processing approaches focused on the single incident. On-demand tools like AI support for PTSD can help you rehearse grounding techniques between clinical sessions in 2026, though they're not a replacement for licensed trauma therapy.
Troubleshooting
- "I have symptoms from both lists" — overlap is normal; let a clinician sort primary diagnosis rather than self-labeling as "both."
- "My trauma was one event but I feel the CPTSD symptoms" — some single incidents (a violent assault, a near-fatal event) can still produce self-concept and regulation symptoms; duration isn't the only variable, severity matters too.
- "I can't pinpoint a start date for my trauma" — common with childhood-origin trauma; approximate is fine, exact dates aren't required for screening.
- "Screening tools feel too clinical to fill out honestly" — try voice journaling instead of written checklists first, then translate patterns into the symptom clusters afterward.
- "I flagged CPTSD but my therapist only treats standard PTSD protocols" — ask directly whether they have ICD-11 CPTSD training; not every trauma therapist does, and that's a fair reason to seek a second referral.
Comparison at a glance
| PTSD | Complex PTSD | |
|---|---|---|
| Trauma origin | Single event | Prolonged or repeated |
| Core clusters | 4 (intrusion, avoidance, mood, arousal) | Same 4, plus 3 more |
| Self-concept | Usually intact | Persistently negative |
| Relationships | Situational avoidance | Chronic trust and closeness difficulty |
| Diagnostic manual | DSM-5, ICD-11 | ICD-11 only (not yet in DSM-5) |
| Typical duration | Weeks to months if treated | Often years without targeted treatment |
Tools and resources
- Polyvagal theory explained — understand the nervous-system mechanics behind hyperarousal
- AI therapy for PTSD and trauma recovery — what daily support looks like alongside clinical care
- A trauma-informed licensed therapist or psychiatrist for formal diagnosis
- The ITQ (International Trauma Questionnaire) if you want a validated CPTSD screening tool before your first appointment
What to do next
If your self-assessment points toward childhood-origin complex trauma, read the deeper breakdown of CPTSD from childhood symptoms and healing steps — it walks through the healing arc in more detail than a single comparison article can.
FAQ
Is Complex PTSD worse than PTSD? Neither is inherently "worse" — CPTSD carries more symptom clusters and tends to take longer to treat because the self-concept and relational damage runs deeper, but severity varies by individual regardless of diagnosis.
Can you have PTSD and CPTSD at the same time? No — ICD-11 treats them as related but distinct diagnoses; a clinician assigns one primary diagnosis based on which symptom cluster set is present, though overlap in early screening is common.
Is Complex PTSD in the DSM-5? Not yet as of 2026 — the DSM-5 recognizes PTSD but not CPTSD as a separate category; ICD-11, used more widely outside the US, added CPTSD in 2019.
What causes Complex PTSD specifically? Prolonged or repeated trauma causes it — childhood abuse, long-term domestic violence, captivity, or trafficking are the most common origins, as opposed to the single-incident trauma behind standard PTSD.
How long does it take to heal from Complex PTSD? There's no fixed timeline; because the trauma was prolonged, treatment is typically longer than standard PTSD care, often spanning a year or more of consistent therapeutic work.
Can AI therapy help with PTSD or CPTSD? AI voice tools like Lovon can support grounding techniques and daily emotional regulation between sessions, but neither PTSD nor CPTSD should be diagnosed or treated by an app alone — licensed clinical care remains the primary treatment path in 2026.
What's the fastest way to tell them apart? Check trauma duration first: one event points to PTSD, a repeated or prolonged pattern points toward CPTSD, then confirm against the three additional self-organization symptoms unique to CPTSD.
Do children get diagnosed with CPTSD differently than adults? The diagnostic criteria are the same across ages, but childhood-origin CPTSD often shows up with more pronounced attachment and self-concept disruption because the trauma occurred during formative relational development.
One last thing
The detail most people miss: CPTSD's negative self-concept symptom isn't just low self-esteem — it's a fixed belief that you are permanently damaged or fundamentally different from other people, and that belief often survives even after the flashbacks and hypervigilance fade. Treating the visible PTSD symptoms without addressing that underlying belief is why some people report feeling "technically better but still broken" years into treatment.
Related guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles

Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
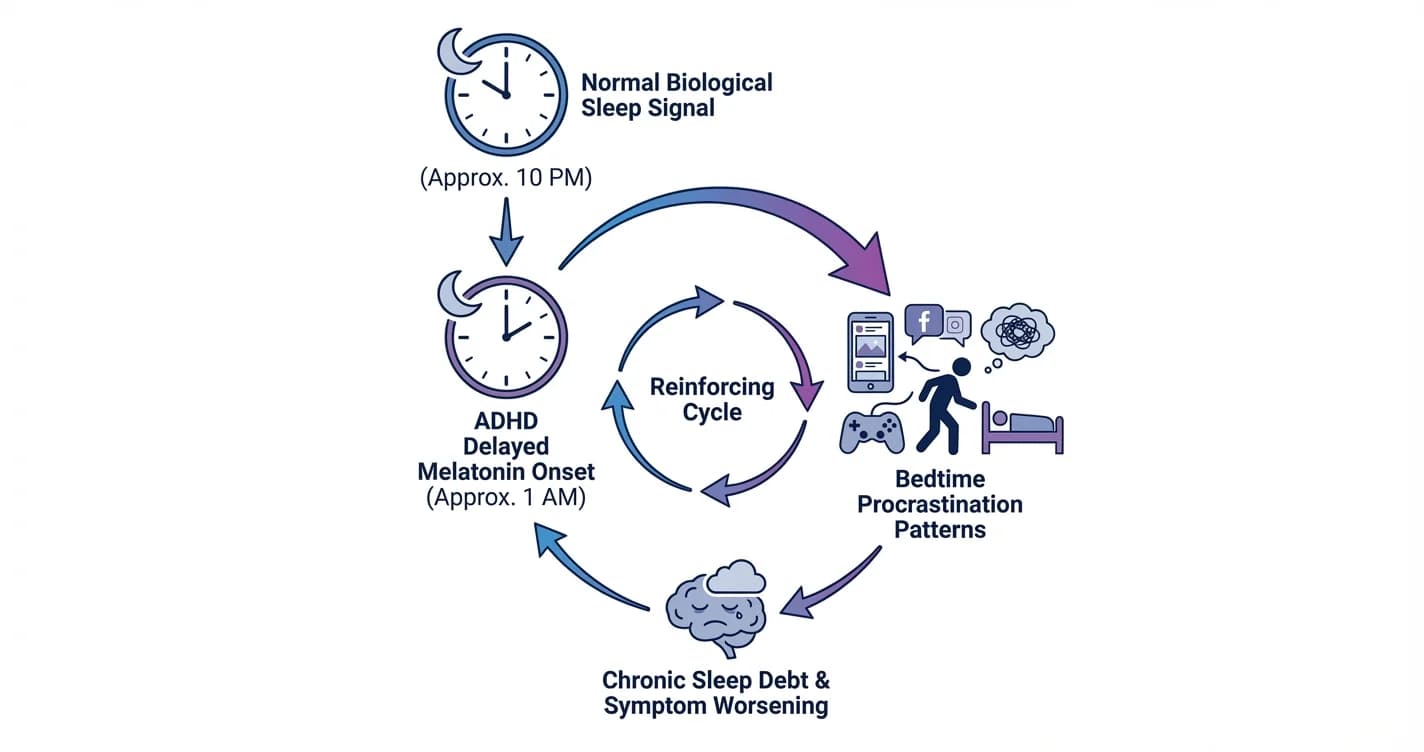
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
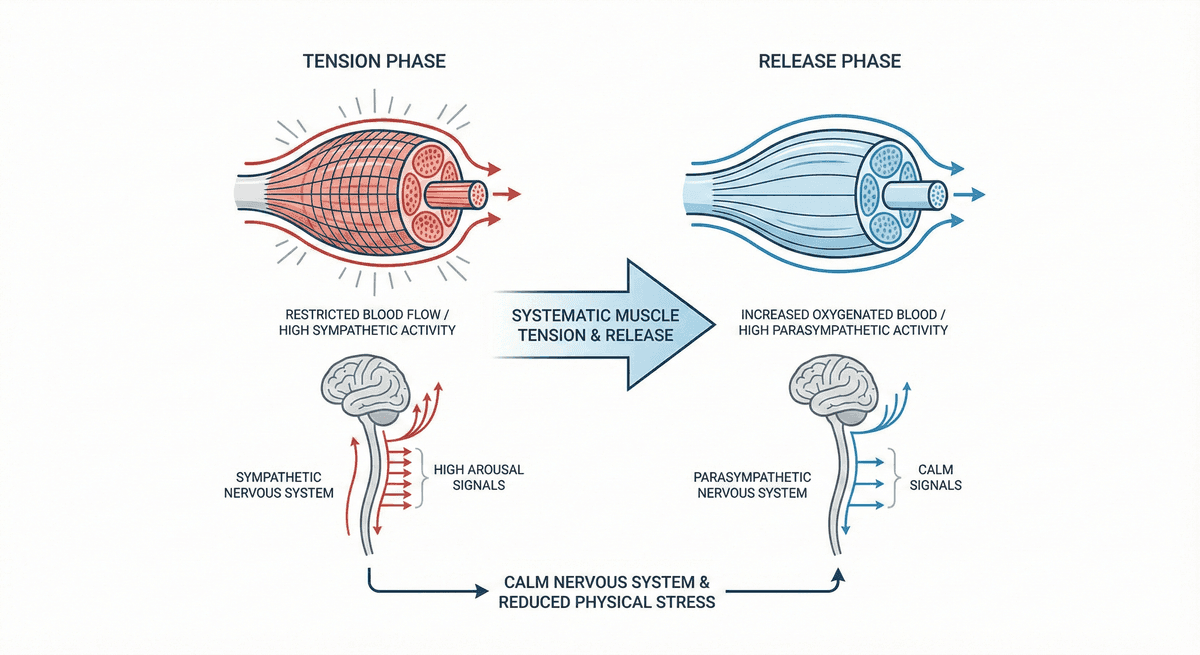
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.