Can You Pass Out from a Panic Attack? (2026)
Can you pass out from a panic attack? Almost never — learn the real biology, why dizziness happens, and 7 steps to manage panic attacks in 2026.
Key Takeaways
- A quiet space or a place where you can sit or lie down safely
- 5–10 minutes of uninterrupted time to practice the techniques
- A basic understanding of why panic attacks feel like fainting (covered in the next section)
- Optional: a journal or voice memo app for tracking triggers after the episode
- [Breathing exercises for anxiety relief](https://lovon.app/blog/anxiety/breathing-exercises-for-anxiety-relief) —
Panic attacks are frightening enough on their own — but the fear of losing consciousness during one is one of the most common questions people ask in 2026. The short answer is clear: passing out from a panic attack is extremely rare, and the biology of a panic attack actually works against fainting. Here is what is really happening in your body, why it feels like you might black out, and what to do instead.
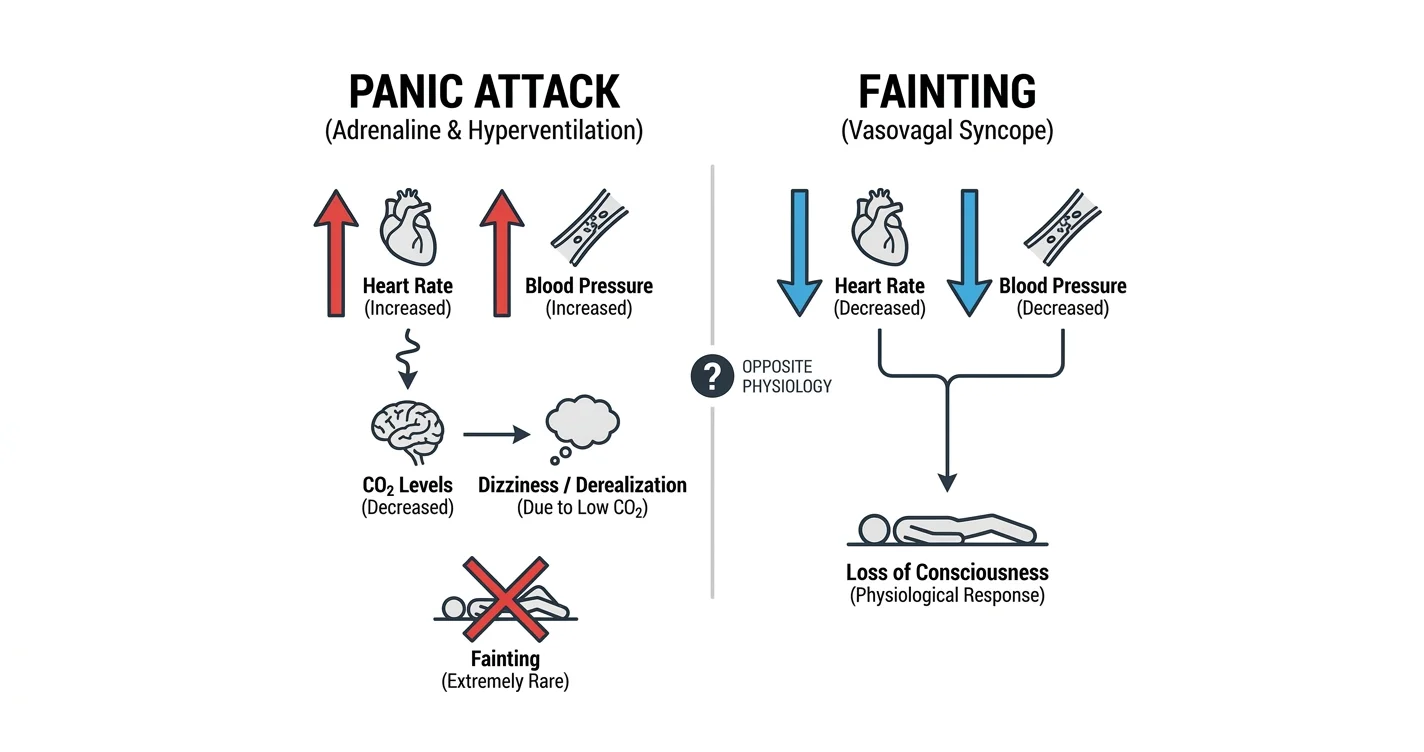
TL;DR: Can you pass out from a panic attack? Almost never. During a panic attack, your blood pressure and heart rate spike — the opposite of what causes fainting. Symptoms like dizziness, tunnel vision, and feeling detached are real and terrifying, but they are driven by hyperventilation and adrenaline, not blood pressure collapse. Learning this distinction is one of the fastest ways to break the fear-panic cycle in 2026. If you do faint, something other than a panic attack is likely the cause and needs medical evaluation.
Why this matters
About 11% of adults in the United States experience at least one panic attack each year. The sensation of impending doom — including the conviction that you are about to pass out — is one of the defining features. When you believe fainting is imminent, the fear intensifies the attack. Breaking that loop starts with understanding what is physically impossible during a standard panic attack and what to do when the symptoms hit.
What you'll need
Before working through the steps below, have these ready:
- A quiet space or a place where you can sit or lie down safely
- 5–10 minutes of uninterrupted time to practice the techniques
- A basic understanding of why panic attacks feel like fainting (covered in the next section)
- Optional: a journal or voice memo app for tracking triggers after the episode
No equipment is required. These techniques work anywhere — at home, at work, on transit.
Why fainting and panic attacks work in opposite directions
Fainting — technically called vasovagal syncope — happens when blood pressure drops suddenly, reducing blood flow to the brain. Your body responds by shutting you down briefly so you can recover horizontally.
A panic attack does the opposite. Adrenaline floods your system. Heart rate climbs — often to 120–160 beats per minute. Blood pressure rises. Blood is actively being pushed to your muscles, not away from your brain. That is why, physiologically speaking, a panic attack is a poor fainting mechanism.
The confusion comes from hyperventilation. When you breathe fast and shallow, carbon dioxide levels drop in your blood. Low CO2 causes blood vessels to constrict slightly — including in the brain. That produces real dizziness, tingling in the hands and face, visual narrowing, and a sense of unreality (called derealization). None of these mean your blood pressure is collapsing. They mean you are breathing too fast.
The one genuine exception: if you have a specific phobia of blood or injury (called blood-injection-injury phobia), your nervous system can produce a two-phase response that does drop blood pressure. This is not a panic attack — it is a distinct physiological reflex. If you consistently faint at the sight of blood, see a doctor; that condition has its own treatment path.
The steps — what to do during a panic attack when you fear passing out
Step 1: Name what is happening
The moment you feel dizziness or the fear of blacking out, say it plainly to yourself: "This is a panic attack. My blood pressure is rising, not falling. I cannot faint from this." This is not wishful thinking — it is accurate physiology. Naming the experience activates the prefrontal cortex and begins to dampen the amygdala's alarm signal. In 2026, cognitive reappraisal during acute anxiety is one of the best-supported techniques in clinical literature. The common mistake here is trying to convince yourself you are "fine" — you are not fine, but you are also not in danger of losing consciousness.
Step 2: Sit or brace, but do not lie down
If you genuinely feel lightheaded, sit with your back supported or brace yourself against a wall. Do not lie flat unless you have already fainted — lying flat during hyperventilation can sometimes make derealization worse because the visual cues change. Sitting keeps you grounded and in contact with a stable surface. The expected outcome: within 20–30 seconds of sitting, the sense of floating usually diminishes because proprioceptive feedback (your body knowing where it is in space) stabilizes.
Step 3: Slow your breathing — specifically extend the exhale
This is the single most direct intervention for the dizziness caused by hyperventilation. Inhale for 4 counts through your nose, then exhale for 6–8 counts through pursed lips or through your nose. The extended exhale activates the parasympathetic nervous system and begins to raise CO2 back toward normal levels. Do this for at least 3 minutes — CO2 normalizes gradually, not instantly. The common mistake: taking one slow breath, feeling no immediate change, and then breathing fast again. The fix requires sustained slow breathing, not a single cycle. For a full guided breakdown of this technique, breathing exercises for anxiety relief covers every variation with step-by-step instructions.
Step 4: Ground yourself with the 5-4-3-2-1 method
Derealization — that "am I real right now" feeling — is the symptom most commonly confused with pre-fainting. Grounding interrupts it by redirecting attention to concrete sensory input. Name 5 things you can see, 4 you can touch, 3 you can hear, 2 you can smell, 1 you can taste. This works because it forces the brain to switch from internal catastrophic prediction to external sensory processing. Each step takes about 30 seconds. By the time you finish all 5 categories — roughly 2–3 minutes — most people report a measurable drop in the intensity of the episode.
Step 5: Let the peak pass without fighting it
Panic attacks peak within 10 minutes in the vast majority of cases and fully subside within 20–30 minutes. Fighting the sensation — tensing up, pacing, Googling symptoms mid-attack — prolongs the adrenaline response. The instruction here is deliberately passive: breathe slowly, stay seated, and observe the symptoms without adding fear on top of fear. Anxiety researcher Claire Weekes called this "floating" — letting the wave move through rather than crashing against it. The common mistake is interpreting the continued presence of symptoms as evidence that something is wrong. Symptoms continuing for 10 minutes is normal; it is not a sign you are about to collapse.
Step 6: After the attack — log what happened
Within an hour of the episode ending, note: what triggered it, what the first symptom was, how long it lasted, and what helped most. Over time, this log reveals patterns. Many people in 2026 use voice journaling for this — speaking the account aloud rather than writing it, which is faster and often feels less clinical. Voice journaling to reduce anxiety daily explains how to structure these entries so they become useful data rather than just venting.
Step 7: Decide whether to seek clinical support
A single panic attack does not require professional intervention. Recurring attacks — especially those that start shaping your behavior (avoiding places, situations, or activities where they happened) — are the clinical threshold for panic disorder. At that point, Cognitive Behavioral Therapy (CBT) has the strongest evidence base, with response rates above 70% in multiple large trials. If cost or access is a barrier, how much is therapy without insurance in 2026 breaks down realistic price ranges and low-cost alternatives. Lovon is not a replacement for clinical care, but it is available anytime between sessions for the kind of between-appointment support that is hardest to access.
Troubleshooting — when the steps do not seem to work
You are still dizzy after 10 minutes of slow breathing. Check whether you are actually slowing down or just thinking you are. Use a timer. Count out the 4-count inhale and 6-count exhale to an actual clock. Perceived slow breathing is often still faster than physiological slow breathing.
The 5-4-3-2-1 grounding makes the derealization worse. Some people find sensory focus increases self-monitoring during an attack. Switch to a physical grounding technique instead: hold something cold (ice, a cold drink), feel the texture of a rough surface, or press your feet flat on the floor with deliberate pressure.
You feel your heart pounding and it scares you more. You are checking your pulse mentally, which amplifies the sensation. Shift attention outward — look at an object across the room and describe it in detail (color, shape, shadow). Heart rate during a panic attack is not dangerous in otherwise healthy people, but the monitoring behavior feeds the loop.
You always fear fainting in specific places (elevators, crowds, heat). This is anticipatory anxiety building a phobia. Each avoidance episode reinforces it. Graduated exposure — entering the feared situation in small controlled doses — is the evidence-based fix, best done with a therapist. AI therapy for anxiety and panic attacks covers how digital tools support between-session exposure practice.
You actually did faint. A genuine loss of consciousness is not a panic attack symptom. Get a cardiac and neurological evaluation. Vasovagal syncope, arrhythmias, hypoglycemia, and orthostatic hypotension all need to be ruled out.
Every attack convinces you that this time is different, this time is dangerous. This is the core cognitive distortion in panic disorder. Write down after each attack: did I faint? The answer, over dozens of attacks, will consistently be no. That record becomes evidence you can use in the next episode.
Tools and resources
- Breathing exercises for anxiety relief — technique library for the slow-exhale method and box breathing
- AI therapy for anxiety and panic attacks — how Lovon supports panic management between clinical sessions
- Coping tools for stress — what works and what does not — evidence ratings for common anxiety interventions
- Lovon — on-demand voice conversations with an AI built around mental health support, available any time a panic episode starts or after one ends
FAQ
Can you pass out from a panic attack? Almost never. Panic attacks raise blood pressure and heart rate — fainting requires blood pressure to drop. The dizziness and tunnel vision you feel are caused by hyperventilation lowering CO2, not by reduced blood flow to the brain.
What does it feel like right before fainting versus a panic attack? Actual pre-faint (vasovagal) starts with warmth, pallor, nausea, and a slow graying of vision — and usually follows a specific trigger like seeing blood or standing up suddenly. A panic attack starts fast, peaks within 10 minutes, and involves racing heart, chest tightness, and fear without the gradual color drain.
How long does a panic attack last? Most peak within 10 minutes. The full episode — including the adrenaline washout — typically resolves within 20–30 minutes. Attacks that last over an hour are atypical and worth discussing with a clinician.
Is it dangerous to have a panic attack alone? For otherwise healthy people, no. The experience is distressing but not medically dangerous. If you have a known heart condition or have never had your symptoms evaluated, getting one medical check is worth it — if only to have confirmed evidence to draw on during future attacks.
What causes the tingling in hands and face during a panic attack? Hyperventilation drops CO2 in the blood. Low CO2 causes mild vasoconstriction and changes ion balance in nerve cells, producing tingling and numbness — especially in the hands, lips, and face. It is uncomfortable and alarming but resolves once breathing normalizes.
Is there medication for panic attacks? Yes. SSRIs and SNRIs are first-line for recurring panic disorder. Benzodiazepines are sometimes prescribed for acute episodes but carry dependency risk. Any medication decision belongs with a licensed psychiatrist or prescribing clinician, not an app.
Can panic attacks get worse over time without treatment? They can — specifically, avoidance behaviors compound. Each time you leave a situation because of a panic attack, the association between that place and danger strengthens. In 2026, untreated panic disorder is one of the leading drivers of agoraphobia.
How is high-functioning anxiety different from panic attacks? High-functioning anxiety is a persistent background state — constant worry, overachievement, and hypervigilance — without necessarily producing acute panic episodes. Panic attacks are discrete, intense, and time-limited. Many people have both. High-functioning anxiety — signs you might be missing covers the overlap in detail.
One last thing
In 2026, the most underused tool for panic attacks is the after-attack debrief — not therapy, not medication, just writing down what happened and what the outcome was. Over 6–8 attacks logged with honest outcomes, most people discover the evidence they have been looking for: the attack was terrifying every time, and they did not faint once. That record, built from your own experience, is more persuasive to a panicking brain than any reassurance from the outside.
Related guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
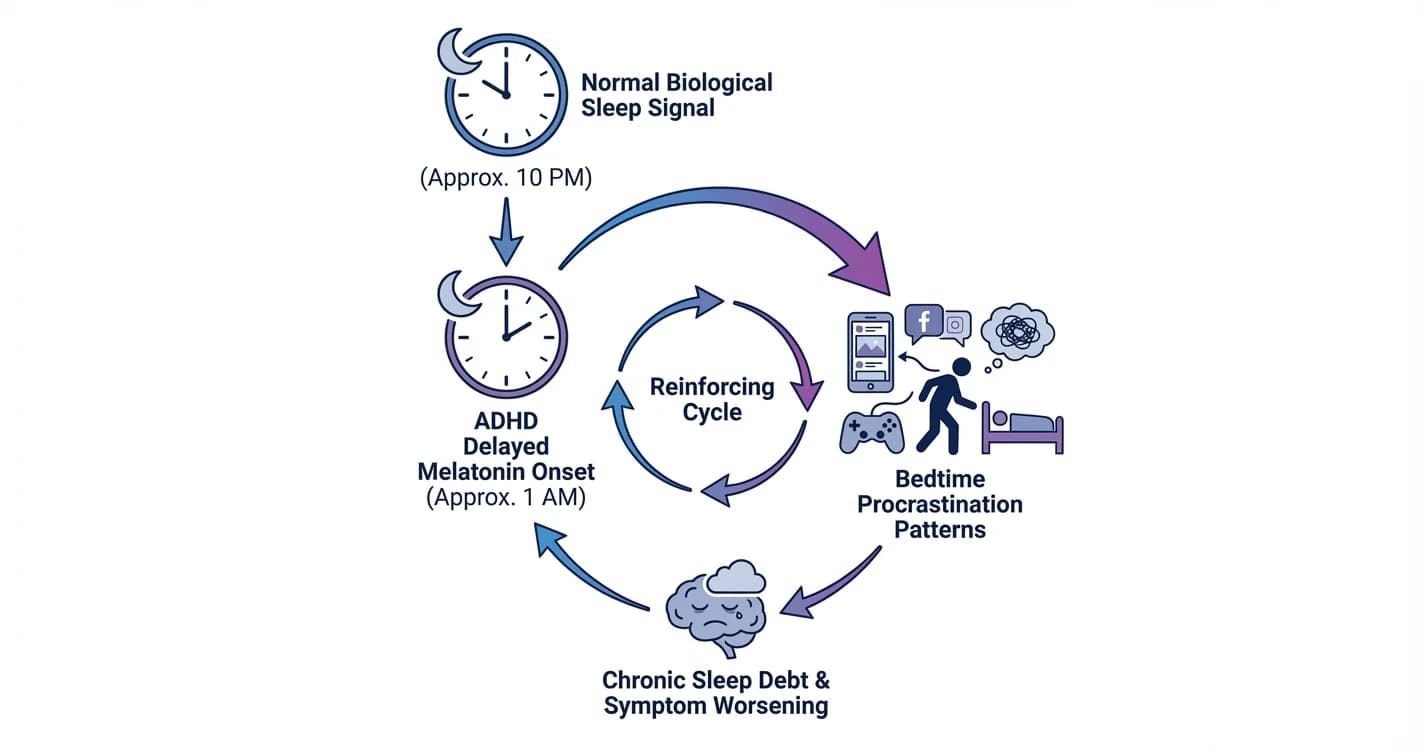
ADHD Sleep Cycle Disruption: Melatonin Delay and Bedtime Procrastination Patterns
Understanding how attention regulation difficulties interfere with natural sleep timing and the nightly wind-down process
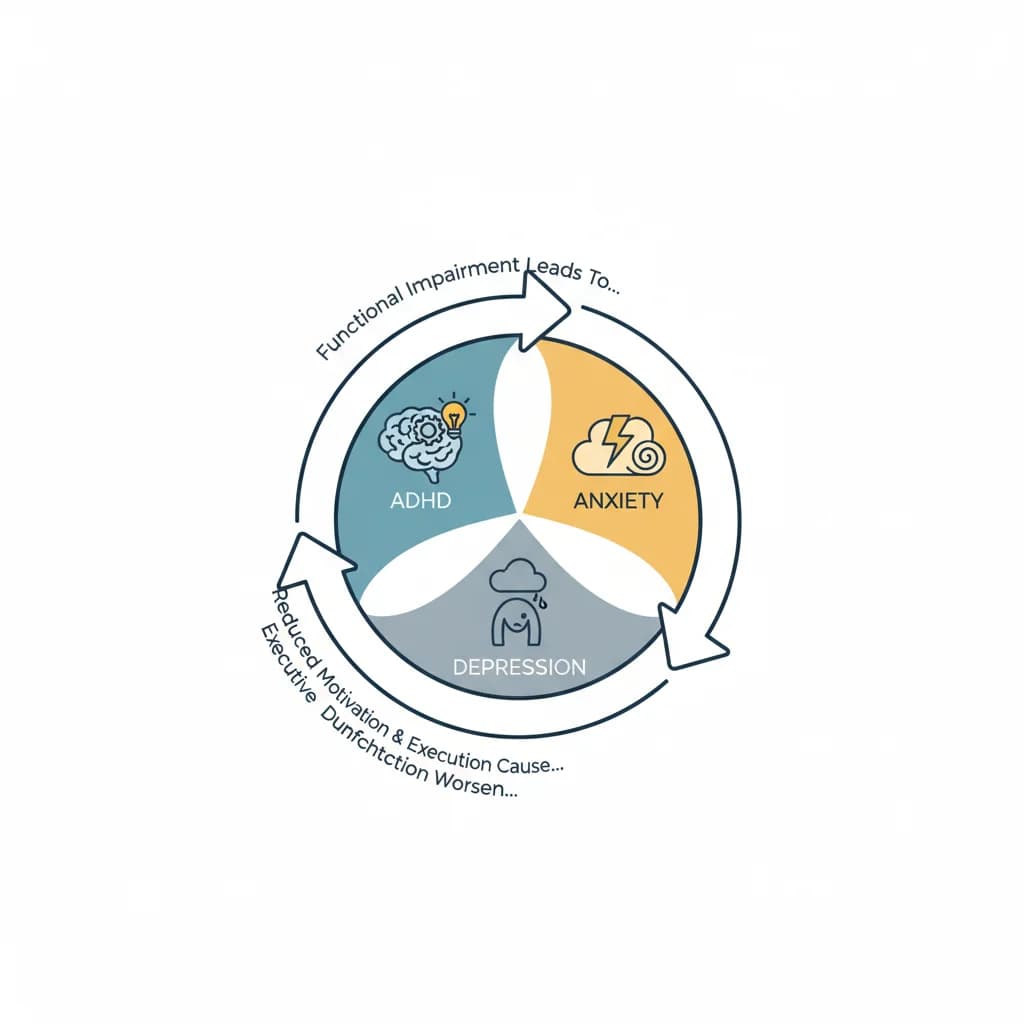
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.