Functional Depression: Signs You're Not Just Tired (2026)
Functional depression keeps you going while draining everything. Learn the 8 signs, how it differs from burnout, and what to do about it in 2026.
Key Takeaways
- 10–15 minutes of honest reflection — no distractions
- A note-taking app or journal — patterns become visible when you write them down
- Willingness to be specific — vague answers produce vague insight
- An open line to professional support — a licensed therapist or psychiatrist for diagnosis and treatment planning,
- An on-demand support tool between sessions — apps like [Lovon](https://lovon.app/) provide voice-based emotional
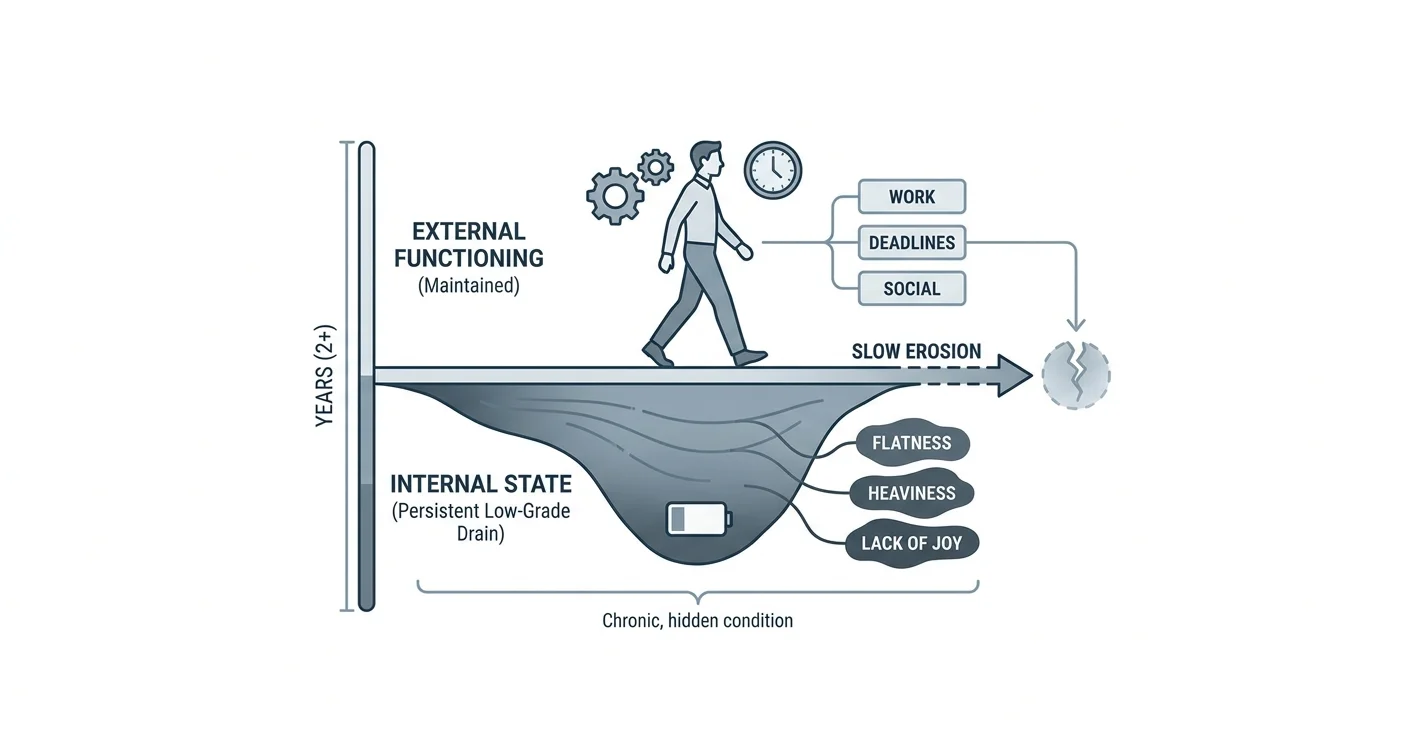
Functional depression is one of the most commonly missed mental health conditions — not because it is rare, but because the people who have it keep showing up. They go to work, meet their deadlines, answer their texts, and look fine from the outside. Inside, something is consistently off: flat, heavy, and hard to name.
TL;DR: Functional depression (also called dysthymia or persistent depressive disorder) is a low-grade, long-lasting form of depression that lets you keep going while quietly draining your energy, motivation, and sense of self. If you have felt "not quite right" for more than two years — not devastated, just dulled — this is what it looks like and what you can do about it in 2026.
Why this matters
Functional depression does not look like the depression most people picture. There is no dramatic collapse. There is just a slow erosion. Research published in the Journal of Affective Disorders found that dysthymia often goes undiagnosed for 5 to 10 years precisely because sufferers appear high-functioning. The cost is real: chronic low mood affects decision-making, relationships, physical health, and the ability to feel genuine pleasure in anything — even good things.
Knowing what you are dealing with is the first step to getting out of it.
What you'll need
Before working through the recognition and response steps below, a few things will help:
- 10–15 minutes of honest reflection — no distractions
- A note-taking app or journal — patterns become visible when you write them down
- Willingness to be specific — vague answers produce vague insight
- An open line to professional support — a licensed therapist or psychiatrist for diagnosis and treatment planning, especially if symptoms have lasted more than two years
- An on-demand support tool between sessions — apps like Lovon provide voice-based emotional support when professional appointments are not available
The steps
Step 1: Distinguish "just tired" from a pattern
Tiredness from a hard week is self-limiting — rest fixes it. Functional depression does not resolve with a weekend off. The diagnostic threshold for persistent depressive disorder (PDD), the clinical name for what most people call functional depression, is a depressed mood present for most of the day, more days than not, for at least 2 years in adults.
Ask yourself: Has this been my baseline for longer than I can remember? If the answer is yes, you are not just tired.
Common mistake: Attributing a 3-year emotional flatness to "personality" or "stress" and never questioning it. Flatness that old is a symptom, not a character trait.
Step 2: Check the six core signs
The DSM-5 criteria for persistent depressive disorder require a depressed mood plus at least two of the following six symptoms, persisting for two or more years:
- Poor appetite or overeating
- Insomnia or sleeping too much
- Low energy or fatigue
- Low self-esteem
- Poor concentration or difficulty making decisions
- Feelings of hopelessness
You do not need all six. Two is enough to meet the clinical bar alongside chronic low mood. Write down which ones apply and how long they have been present. Specificity here matters when you eventually talk to a clinician.
Expected outcome: A clearer picture of whether your experience fits the pattern — not a self-diagnosis, but a starting framework.
Step 3: Map the hidden signs that people miss
Beyond the clinical checklist, functional depression shows up in subtler ways that are easy to rationalize:
- Joylessness in things you used to enjoy — hobbies feel like obligations, time with friends feels like effort
- Chronic low-grade irritability — not rage, just a short fuse that surprises you
- Anhedonia on autopilot — you do things but feel nothing doing them
- Guilt about not feeling worse — "I have nothing to be depressed about" is a thought that keeps many people from seeking help
- Social withdrawal that looks like introversion — you cancel plans not to recharge but to avoid the effort of being present
- A persistent sense that something is wrong but you cannot name it
Functional depression is skilled at disguising itself as personality. That disguise is the problem.
Common mistake: Waiting until you feel "bad enough" to do something. Functional depression rarely reaches a dramatic low — it just stays. Waiting for a crisis that may never come means living below your baseline for years.
Step 4: Rule out the look-alikes
Several other conditions can produce a similar profile. Before assuming functional depression, consider whether these fit better:
- Burnout — linked to a specific context (job, caregiving role). Burnout improves when the stressor is removed. Functional depression does not.
- Hypothyroidism — fatigue, low mood, weight changes. A simple blood panel rules this in or out. Worth checking before any mental health label.
- Seasonal Affective Disorder (SAD) — mood follows a seasonal cycle, typically worsening in winter and lifting in spring. Functional depression is year-round.
- High-functioning anxiety — high-functioning anxiety can mimic the flat, exhausted presentation of functional depression, especially when anxiety manifests as emotional numbing rather than panic.
These are not mutually exclusive. Functional depression and anxiety co-occur frequently — one 2026 clinical review placed the comorbidity rate above 60%.
Expected outcome: A cleaner hypothesis to bring to a clinician, rather than a jumbled list of symptoms.
Step 5: Start a daily mood log for two weeks
Two weeks of data does more than two minutes of reflection. Each day, record:
- Morning mood (1–10) — before screens, before coffee
- Afternoon mood (1–10)
- One thing you noticed about your energy or motivation
- One thing you avoided that you intended to do
This log serves two purposes. First, it surfaces patterns you cannot see in the moment — most people with functional depression score between 3 and 5 consistently, rarely spiking or crashing. Second, it gives a clinician concrete evidence rather than a vague "I've been feeling off."
Common mistake: Abandoning the log after three days because it feels pointless. That feeling — "why bother" — is itself a data point.
Step 6: Get a clinical assessment
A mood log and a symptom checklist are useful, but they are not a diagnosis. Persistent depressive disorder is diagnosed by a licensed mental health professional using structured clinical interviews. In 2026, you have more access options than at any previous point:
- In-person psychiatrist or psychologist — gold standard for complex presentations
- Telehealth therapy platforms — same clinical rigor, no commute; costs vary significantly depending on insurance
- Primary care physician — can conduct an initial PHQ-9 screening and refer
If cost is a barrier, the therapy cost guide for 2026 covers current out-of-pocket ranges and low-cost options.
Expected outcome: An actual diagnosis, or a clear ruling-out, plus a treatment direction — typically a combination of psychotherapy (especially CBT or behavioral activation) and, where appropriate, medication.
Step 7: Build a between-session support structure
Clinical treatment for functional depression works best when it is reinforced between sessions. Therapy once a week is 1 hour out of 168. What happens in the other 167 matters.
Practical between-session tools:
- Behavioral activation — scheduling one small, concrete activity per day that used to bring pleasure, even if it feels hollow at first. The behavior precedes the feeling.
- Voice journaling — speaking your thoughts aloud activates processing differently than typing. Apps like Lovon let you talk through what you are carrying in real time, any time.
- Reducing cortisol load — chronic low-grade depression is closely tied to sustained cortisol elevation. Sleep regularity, reduced alcohol, and brief daily movement all lower the baseline. See the guide to reducing cortisol naturally for specific steps.
- Social engagement on a schedule — motivation will not show up first. Commitment to one social contact per week, regardless of mood, creates a structure motivation can eventually follow.
Common mistake: Waiting to feel motivated before doing any of the above. Functional depression specifically impairs motivation. You act first; the motivation catches up later.
Step 8: Reassess at 60 days
At the 60-day mark, return to your original mood log and the six-symptom checklist. Specifically look for:
- Has your average daily mood score shifted by 1 or more points?
- Are any of the six symptoms less frequent or less intense?
- Are you completing more of your intended daily activities?
Progress with functional depression is slow and non-linear. A 1-point average improvement over 60 days is clinically meaningful. If nothing has shifted after a structured 60-day effort that includes professional support, tell your clinician — it may indicate the treatment approach needs adjustment, the diagnosis needs review, or an underlying medical factor has not been addressed.
Troubleshooting
"I've had this my whole life — is it even treatable?" Yes. Persistent depressive disorder responds to both psychotherapy and medication. Early-onset (before age 21) is associated with longer episodes, but treatment still works. Duration of suffering is not a measure of treatability.
"My therapist says I'm fine." If you had a single session and described surface-level functioning, a clinician may not have seen the full picture. Be explicit: tell them how long the flatness has lasted, use the word "dysthymia," and share your mood log. Clinical assessment depends on what you disclose.
"I tried antidepressants and they didn't help." Medication response for persistent depressive disorder is often slower than for major depressive disorder, and the first medication tried is not always the right one. This warrants a follow-up conversation with a psychiatrist, not a conclusion that medication cannot work for you.
"I can't afford therapy right now." Low-cost and sliding-scale options exist through community mental health centers, university training clinics, and open-access platforms. Check current pricing and availability via the 2026 therapy cost guide — options have expanded compared to prior years.
"I feel guilty about struggling when my life looks fine." This thought is a symptom of functional depression, not an accurate read of your situation. Depression does not require visible hardship as a prerequisite. The guilt itself often keeps people from seeking help for years.
"I'm not sure if this is depression or just my personality." If you can point to a period in your past — even briefly — when you felt genuinely lighter, more interested, more yourself, that contrast is meaningful. A baseline that predates the flatness suggests a condition, not a character.
Tools and resources
- AI therapy for depression support — how AI-assisted sessions work for depressive symptoms
- Free AI therapist for depression — on-demand voice support for days when professional help is not accessible
- Coping tools for stress: what works and what does not — evidence-grounded overview of coping strategies
- Lovon voice therapy app — talk through what you are feeling anytime, built with input from PhD psychologists
- Your primary care physician — first stop for ruling out thyroid and other medical causes
- Licensed therapist or psychiatrist — required for formal diagnosis and treatment planning
What to do next
If this article confirmed something you have suspected for a while, the most useful next move is a clinical assessment — not more reading. Book a session with a licensed therapist or your primary care doctor this week. While you wait for that appointment, Lovon is available to help you process what you are feeling without a waitlist.
FAQ
What is functional depression? Functional depression is an informal term for persistent depressive disorder (dysthymia) — a chronic, low-grade form of depression that allows a person to maintain daily responsibilities while experiencing sustained low mood, low energy, and reduced enjoyment of life for two or more years.
How is functional depression different from regular depression? Major depressive disorder ("regular" depression) typically involves more severe episodes that can prevent daily functioning. Functional depression is less intense but longer-lasting — often 5 to 10 years before diagnosis — and harder to recognize because the person keeps functioning.
Can you have functional depression and not know it? Yes. This is the most common pattern in 2026. Because the person is coping and appears fine, neither they nor the people around them identify it as depression. The flatness gets attributed to personality, stress, or life circumstances.
What causes functional depression? No single cause. Contributing factors include genetics, early adverse experiences, chronic stress, certain medical conditions (particularly thyroid disorders), and prolonged periods of emotional suppression. Most cases involve a combination.
How long does functional depression last without treatment? Without treatment, persistent depressive disorder averages over 5 years in duration. Some people experience it for decades. Treatment significantly shortens episode length and reduces the likelihood of developing a major depressive episode on top of it — a pattern called "double depression."
Is functional depression a real diagnosis? Yes. It is listed in the DSM-5 as Persistent Depressive Disorder (PDD) and in the ICD-11 as Dysthymia. The informal term "functional depression" is not a clinical label, but it describes the same condition in plain language.
Can an app help with functional depression? An app is not a substitute for clinical care, but it can provide consistent emotional support, coping practice, and self-reflection between therapy sessions. In 2026, voice-based AI tools designed with psychological input — like Lovon — are used by many people to bridge the gap between weekly appointments.
When should I see a doctor about functional depression? If your low mood has lasted more than a few months and is not explained by a specific life event, see a clinician. Do not wait for a crisis. Functional depression responds to treatment, and the sooner it is addressed, the shorter the episode.
One last thing
People with functional depression are often praised for their resilience. They are the ones who "always show up," "handle everything," "never complain." That praise is part of why functional depression stays hidden for so long. Functioning is not the same as being okay. If you have been quietly carrying this for years, that is not a strength to maintain — it is a burden worth putting down.
Related guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
Amygdala Reactivity Reduction: Gray Matter Changes After Eight Weeks of Mindfulness Practice
Discover how eight weeks of mindfulness practice reshapes the brain, reducing amygdala reactivity and building lasting neural resilience.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.