How to Get Out of a Depressive Episode (2026 Guide)
Learn how to get out of a depressive episode on your own with 7 evidence-based steps — from nervous system regulation to behavioral activation and voice-based support.
Key Takeaways
- A phone or device with a timer
- Access to daylight or a window
- A glass of water nearby before you start
- Approximately 10–20 minutes for the early steps; longer steps are broken into segments
- Willingness to act before you feel ready — the feeling follows the action, not the other way around
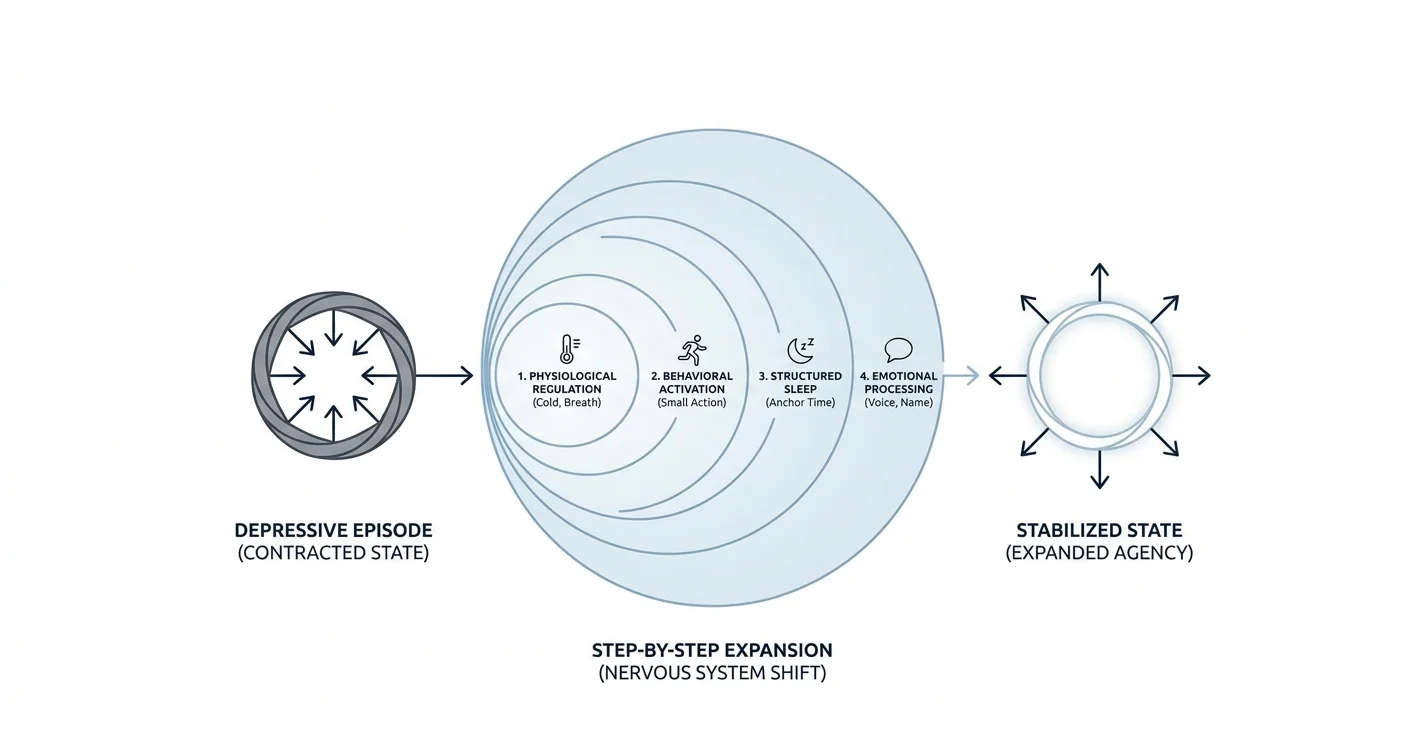
A depressive episode does not announce a clear exit — but there are concrete actions that shift the weight, even on the days when getting out of bed feels like the hardest thing you have done all year. This guide walks you through exactly how to get out of a depressive episode using steps grounded in evidence-based psychology, without requiring you to feel motivated first.
TL;DR: Getting out of a depressive episode on your own in 2026 means working with your nervous system, not against it. Start with the smallest possible physical action — sunlight, a five-minute walk, or cold water on your face — then layer in behavioral activation, structured sleep, and voice-based emotional processing. Depression contracts your world; these steps expand it back, one hour at a time. You will not feel better immediately, but each step measurably shifts your brain chemistry in the right direction.
Why this matters
Depression affects roughly 21 million adults in the United States each year, according to the National Institute of Mental Health. Most episodes — especially mild to moderate ones — do resolve, but waiting passively makes them last longer. The steps below are not a replacement for clinical care if you need it. They are the actions that shorten the episode when you are managing it yourself.
What you will need
- A phone or device with a timer
- Access to daylight or a window
- A glass of water nearby before you start
- Approximately 10–20 minutes for the early steps; longer steps are broken into segments
- Willingness to act before you feel ready — the feeling follows the action, not the other way around
- An honest self-check: if you are experiencing thoughts of self-harm, contact the 988 Suicide and Crisis Lifeline (call or text 988) before doing anything else
The steps
Step 1 — Regulate your body before your mind
What it accomplishes: Depression is not just a thought pattern — it lives in the body. Your heart rate drops, your posture collapses, your breathing gets shallow. Changing your physiology is the fastest route out of the low state, and it requires zero motivation.
How to do it: Splash cold water on your face for 30 seconds, or step outside for two minutes of direct sunlight. If neither is possible, do 10 slow exhalations where the out-breath is twice as long as the in-breath (in for 4 counts, out for 8). This activates the parasympathetic nervous system and creates a brief but real shift in your internal state.
Why it matters: Your prefrontal cortex — the part that plans, reasons, and solves — goes offline when your stress system is dysregulated. You cannot think your way out of depression from that state. You regulate first, then think.
Expected outcome: A small but perceptible reduction in the physical heaviness. Do not expect to feel good. Expect to feel 5% less locked.
Common mistake: Skipping this step because it feels trivial. It is not. It is the unlock for every step that follows.
Step 2 — Name what you are feeling without judgment
What it accomplishes: Affect labeling — putting a name to an emotion — reduces amygdala activation. A 2007 UCLA study published in Psychological Science showed that naming emotions in real time measurably reduced their intensity.
How to do it: Say aloud or write: "Right now I feel _____." Use a specific word: heavy, hollow, numb, tired, hopeless, flat. Do not say "bad" or "depressed" — get precise. Then add: "That makes sense because _____." You are not solving it. You are witnessing it.
Why it matters: When you name the feeling, you shift from being inside the emotion to observing it. That distance is where change starts.
Expected outcome: Mild relief, sometimes accompanied by tears. That is your nervous system releasing pressure.
Common mistake: Jumping straight to "why do I feel this way" before you have named the feeling. Analysis without acknowledgment makes the episode worse, not better.
Step 3 — Use behavioral activation to break the withdrawal loop
What it accomplishes: Depression pulls you toward isolation and inactivity, which deepens the episode. Behavioral activation — doing something small and concrete — interrupts that loop without requiring motivation first.
How to do it: Choose one 5-minute action from this list. Pick the smallest one that applies to where you are right now:
- Make your bed (or straighten one corner of it)
- Drink a full glass of water
- Send one text to someone you trust — it can be just "hey"
- Eat something, even if it is five crackers
- Step outside for 90 seconds
Why it matters: Action precedes motivation in depression — the research on behavioral activation, developed by psychologist Peter Lewinsohn in the 1970s and refined through multiple RCTs since, consistently shows this. Waiting to feel motivated keeps you stuck.
Expected outcome: Completing the action generates a small but real sense of agency. Repeat once more with a different item on the list.
Common mistake: Picking an action that is too large ("I will clean the whole apartment"). The goal is a win, not a project.
Step 4 — Anchor your sleep and wake time
What it accomplishes: Depression disrupts circadian rhythms, and disrupted rhythms deepen depression — it is a feedback loop. Anchoring your sleep schedule breaks it.
How to do it: Set one fixed wake time for the next 7 days and stick to it regardless of when you fell asleep. Even if you slept 4 hours, get up at the same time. Expose yourself to natural light within 30 minutes of waking. Do not nap for more than 20 minutes before 3 p.m.
Why it matters: A 2023 analysis in JAMA Psychiatry found that irregular sleep timing was independently associated with depression severity — even after controlling for total sleep duration. The timing matters as much as the hours.
Expected outcome: Sleep quality typically improves within 5 to 7 days of a consistent schedule. The first two days feel harder before they feel easier.
Common mistake: Staying in bed past your alarm because you did not sleep well. This reinforces the cycle rather than breaking it.
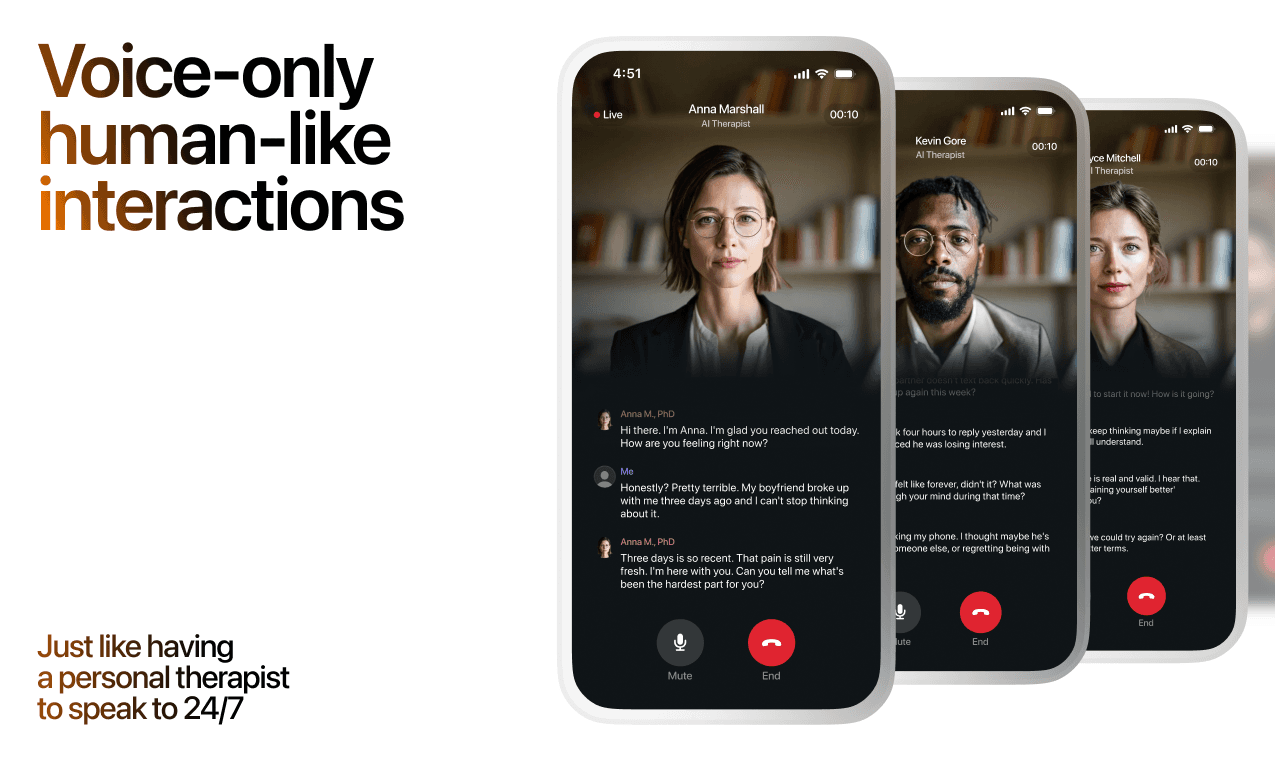
Step 5 — Talk it out — with a person or an AI voice tool
What it accomplishes: Externalizing your thoughts — speaking them out loud — reduces rumination more effectively than writing alone, according to several studies on expressive disclosure. Rumination is one of the key mechanisms that prolongs depressive episodes.
How to do it: Call someone you trust and tell them honestly how you have been feeling. If that feels too hard today, use a voice-based tool to say what is on your mind. Lovon is an AI-powered voice therapy app built with input from PhD psychologists that lets you have a real-time voice conversation about what you are going through — no appointment, no waitlist. It is not a licensed clinician, but it gives you a structured, private space to externalize and process when human support is not immediately available. You can read more about AI therapy for depression support to understand how this kind of tool fits into a broader support plan.
Why it matters: Depression thrives in silence and rumination. Speaking — even to an AI — breaks the echo chamber.
Expected outcome: After 10 to 15 minutes of honest talking, most people report feeling noticeably lighter. The thoughts that felt overwhelming often become more manageable once they are spoken aloud.
Common mistake: Waiting until you feel articulate. You do not need to make sense. Start talking and the sense arrives.
Step 6 — Move your body for 10 minutes
What it accomplishes: Exercise produces immediate neurochemical changes — specifically increases in BDNF (brain-derived neurotrophic factor), dopamine, and endorphins — that reduce depressive symptoms in the short term.
How to do it: Walk for 10 minutes outside. If outside is not possible, put on music and move in your room. The intensity does not matter. The movement does. Set a timer so you are not relying on motivation to stop or continue.
Why it matters: A 2016 meta-analysis in Neuroscience and Biobehavioral Reviews covering 49 studies found that exercise produced a moderate-to-large antidepressant effect. Ten minutes is enough to trigger the acute response.
Expected outcome: A mild but real elevation in mood during or shortly after movement. This is not a cure — it is a lever you pull every day.
Common mistake: Deciding you will exercise "properly" when you feel better. That day does not come on its own. The exercise is what gets you to that day.
Step 7 — Reduce one decision, not all of them
What it accomplishes: Decision fatigue is significantly worse during depression because executive function is impaired. Simplifying even one recurring decision frees up cognitive resources for recovery.
How to do it: Pick one daily decision and automate it for the next 14 days. Eat the same breakfast. Wear the same type of outfit. Set one fixed mealtime. The goal is to reduce cognitive load in one area, not to overhaul your life.
Why it matters: Every unnecessary decision depletes the mental energy you need to do the steps above. In 2026, decision fatigue is well-documented as a recovery barrier in clinical depression literature.
Expected outcome: Marginally less friction in your day. Small, but real.
Common mistake: Trying to restructure your entire routine at once. One decision. One change.
Troubleshooting
"I cannot get out of bed at all." Do Step 1 lying down — slow exhales, 8-count out-breath, 10 repetitions. Then sit up. Do not stand yet. Sitting is the first win.
"I have done all of this before and it did not work." If self-directed steps have not shifted a persistent episode, that is clinical information — it means the episode may need professional support. Free AI therapy for depression is one bridge option while you wait for an appointment.
"I am sleeping too much, not too little." Hypersomnia is common in depression. The same anchor-time rule applies: set a fixed wake time, get light immediately, and limit time in bed to 8–9 hours even if you want more.
"I feel worse when I try to talk about it." Some people find direct emotional conversation activating in a painful way early in an episode. Try voice journaling instead — speak without expecting a response. The on-demand emotional support format can help here.
"The motivation to do any of this is zero." This is expected. The steps are sequenced to not require motivation. Start with Step 1 — it requires nothing except being alive and near water or air.
"It has been more than two weeks with no improvement." A depressive episode lasting more than two weeks that has not responded to self-directed tools meets the clinical threshold for evaluation by a licensed provider. This is not a failure — it is a signal.
Tools and resources
- Lovon app — voice conversations with an AI therapist, available anytime, built with PhD psychologist input. See lovon.app for access.
- Best AI app for depression support in 2026 — a breakdown of AI tools specifically built for depression
- How to reduce cortisol levels naturally — directly relevant when stress is compounding the episode
- 988 Suicide and Crisis Lifeline — call or text 988 (US)
- NAMI Helpline — 1-800-950-NAMI (weekdays, 10 a.m.–10 p.m. ET)
What to do next
Once you have stabilized the episode using these steps, the goal shifts from "getting out" to "staying out." That requires understanding the patterns underneath — what triggers your low periods, what your early warning signs are, and what a real support structure looks like for you long-term. A deeper look at how to structure ongoing support is in how to start AI therapy for the first time.
FAQ
How long does it take to get out of a depressive episode on your own? Mild to moderate episodes often lift within 2 to 8 weeks with active self-directed steps. Without any intervention, they can last 3 to 6 months or longer. The steps above shorten the timeline by targeting the biological and behavioral loops that keep episodes running.
What is the fastest way to get out of a depressive episode? Physical regulation first — cold water, breathwork, or sunlight — followed immediately by behavioral activation. These produce the fastest short-term shift because they change neurochemistry directly rather than relying on cognitive change first.
Is it possible to get out of depression without medication? Yes, for many people with mild to moderate depression. Behavioral activation, structured sleep, exercise, and emotional processing are all backed by clinical evidence. Severe or treatment-resistant depression typically requires professional intervention and sometimes medication.
Should I talk to someone during a depressive episode? Yes. Externalizing your thoughts reduces rumination, which is one of the primary mechanisms that prolongs episodes. If you cannot reach someone you trust, a voice-based tool like Lovon gives you a private space to process in real time.
Why does depression make it so hard to do even small things? Depression reduces activity in the prefrontal cortex — the part of the brain responsible for planning, initiation, and motivation — while increasing activity in the amygdala, which processes threat. The result is high internal alarm with low capacity for action. That is not weakness. That is neuroscience.
What foods help during a depressive episode? Omega-3-rich foods (fatty fish, walnuts, flaxseed), fermented foods, and complex carbohydrates are associated with better mood regulation in observational studies. The more practical rule: eat something, even if it is small. Skipping meals worsens mood stability.
When should I see a doctor or therapist for depression? If the episode has lasted more than two weeks, if it is interfering significantly with work or relationships, if you are having thoughts of self-harm, or if self-directed steps have produced no improvement — those are all clear signals for professional evaluation.
Can an AI app actually help with depression? AI tools designed for mental health support — like Lovon — help with emotional processing, building coping habits, and reducing the isolation that worsens depression. They are not a substitute for licensed clinical care in moderate to severe cases, but they provide real, structured support between sessions or when professional access is limited.
One last thing
Depression tells you that nothing will help — and that is one of its most reliable symptoms. The fact that you are reading a guide on how to get out of a depressive episode means some part of you is already pushing back. That part is right. Act on it before the episode convinces you otherwise.
Related guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
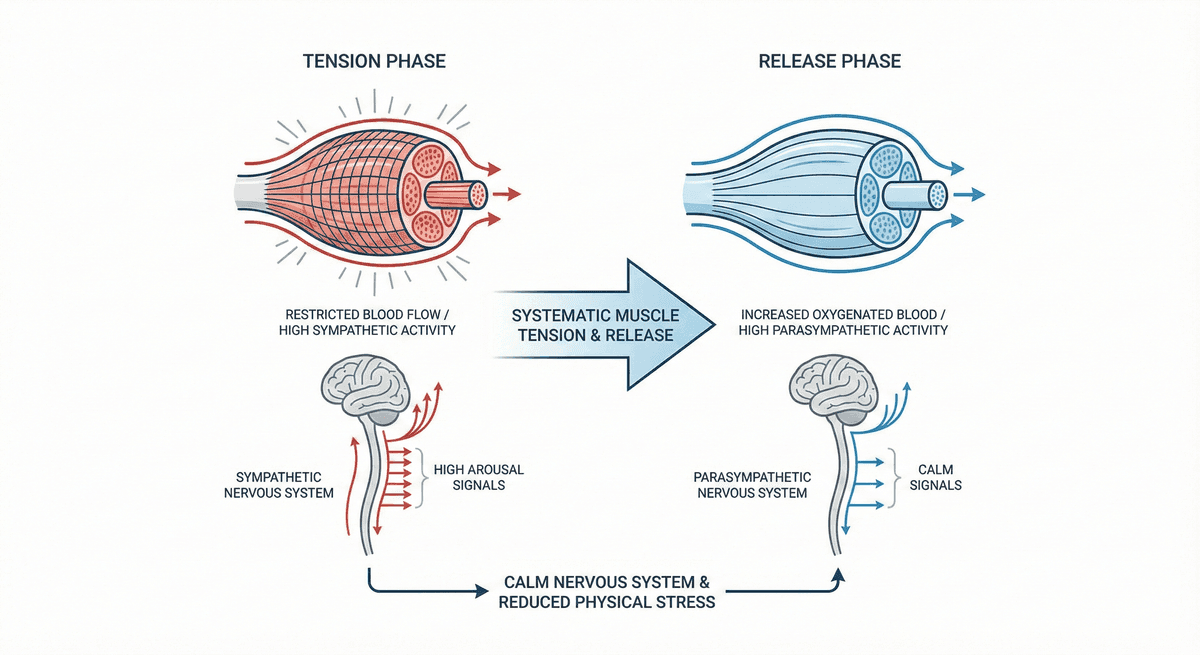
Progressive Muscle Relaxation for Stress Reduction
A systematic muscle group tension and release technique that calms the nervous system and reduces physical stress.
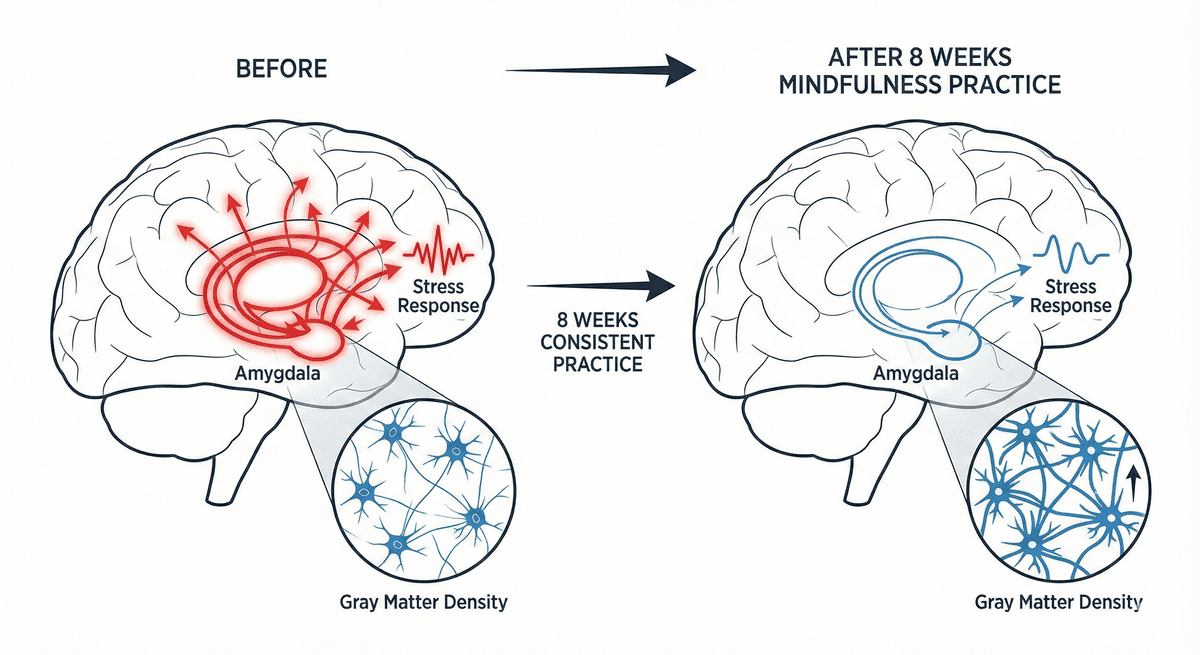
Amygdala Reactivity Reduction: Gray Matter Changes After Eight Weeks of Mindfulness Practice
Discover how eight weeks of mindfulness practice reshapes the brain, reducing amygdala reactivity and building lasting neural resilience.
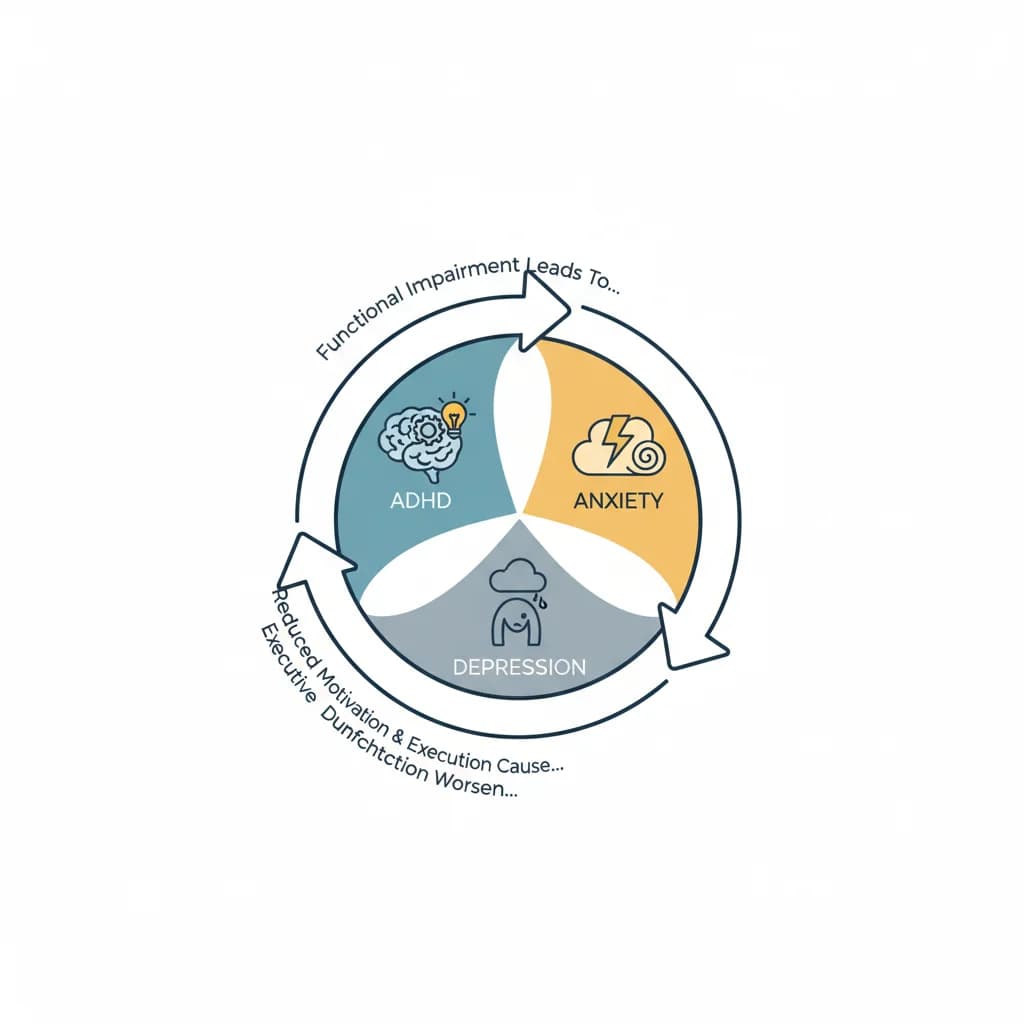
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.