ADHD Rejection Sensitive Dysphoria Explained (2026)
Rejection sensitive dysphoria ADHD causes sudden, intense emotional pain from perceived rejection. Learn what RSD is, why it happens, and 7 steps to manage it.
Key Takeaways
- A basic understanding of what RSD is (covered below)
- Awareness of your personal RSD triggers
- At least one in-the-moment coping tool you trust
- A way to process the emotion after the spike — journaling, voice conversation, or therapy
- Time: most RSD episodes peak within 20–30 minutes, so short interventions work
Rejection sensitive dysphoria ADHD is one of the most painful — and least talked about — parts of living with ADHD. This guide explains what it is, why it happens, and what you can actually do when it hits.
TL;DR: Rejection sensitive dysphoria (RSD) is an intense emotional response to real or perceived rejection that affects an estimated 99% of adults with ADHD, according to ADDitude Magazine's 2026 survey data. The pain is neurological, not a character flaw. It shows up in relationships, work, and friendships, and it's manageable with the right tools — including emotional regulation strategies, therapy, and on-demand support apps like Lovon that let you process the feeling the moment it strikes.
Why This Matters
Most ADHD content focuses on focus and organization. RSD gets skipped because it's hard to measure and easy to mislabel as anxiety, borderline personality disorder, or just being "too sensitive." But for many people with ADHD, rejection sensitivity is the symptom that does the most daily damage — to careers, relationships, and self-worth. Understanding the neuroscience behind it changes how you respond to it.
What You'll Need
Before working through RSD, know what you're dealing with:
- A basic understanding of what RSD is (covered below)
- Awareness of your personal RSD triggers
- At least one in-the-moment coping tool you trust
- A way to process the emotion after the spike — journaling, voice conversation, or therapy
- Time: most RSD episodes peak within 20–30 minutes, so short interventions work
What Is Rejection Sensitive Dysphoria ADHD?
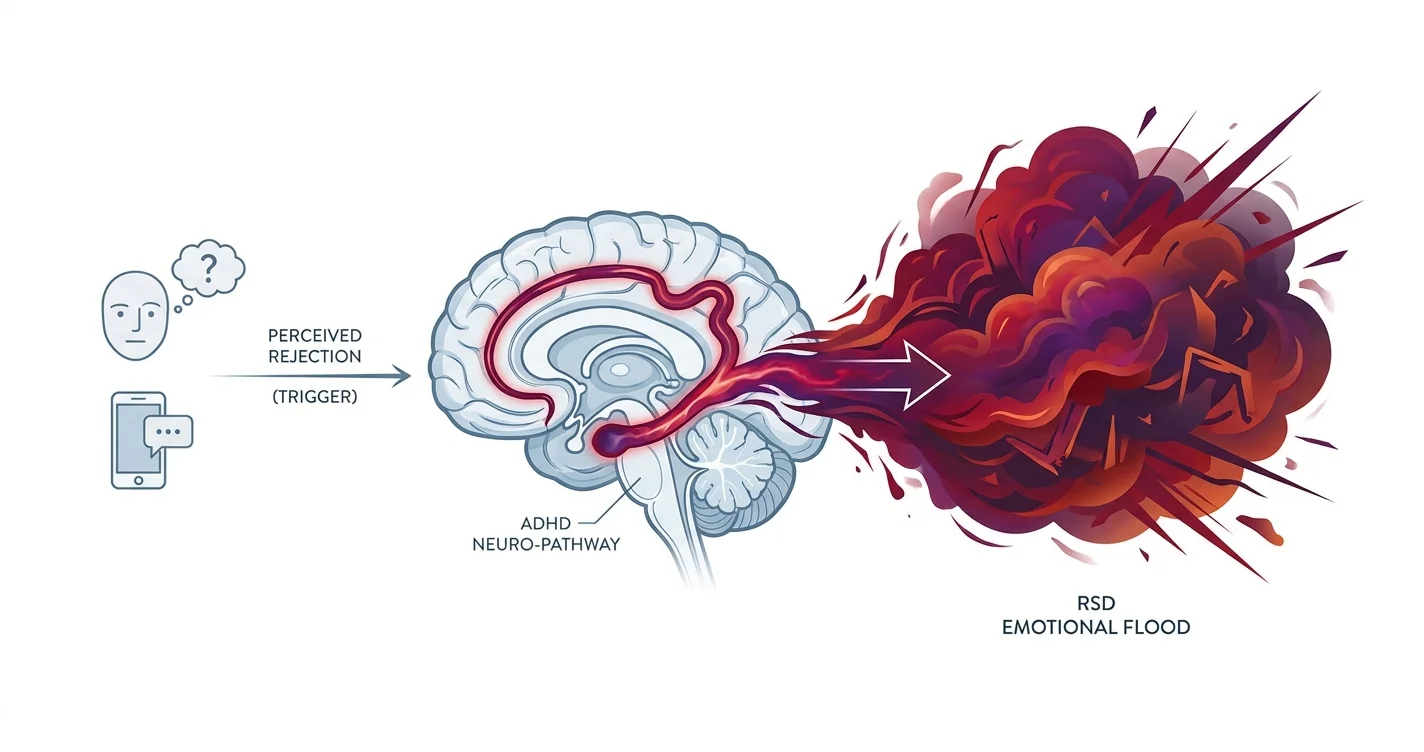
RSD is an extreme emotional reaction — often described as a sudden wave of shame, rage, or despair — triggered by the perception of being rejected, criticized, or falling short of someone's expectations. The key word is perception: the rejection doesn't have to be real. A two-word reply, a missed invitation, or a neutral expression on a colleague's face can set it off.
Dr. William Dodson, a psychiatrist who has worked extensively with ADHD adults, describes the pain of RSD as "the worst emotion I have ever felt" according to his patients — more intense than grief, more physical than anxiety. That's not hyperbole. It's neurological. The ADHD brain regulates emotion differently, and the pathway from stimulus to full emotional flood is much shorter than in a non-ADHD brain.
RSD is not yet listed as a formal DSM-5 diagnosis on its own. It sits under the broader umbrella of emotional dysregulation in ADHD, which affects an estimated 70% of children with ADHD and persists into adulthood for the majority of them.
The Steps: Working Through an RSD Episode
Step 1 — Recognize the trigger before the flood
What it accomplishes: Catching the moment RSD starts gives you a 5–10 second window before the emotional escalation locks in. That window is everything.
RSD triggers fall into three categories: direct rejection (someone says "no"), perceived rejection (someone's tone changes), and anticipatory rejection (you avoid something because you expect rejection). Write down your top 3 personal triggers. Most people have a pattern — it's usually one category that dominates.
Common mistake: Waiting until you're already flooded to try to intervene. At that point, rational thinking is offline. The recognition work has to happen before or right at the start.
Step 2 — Name it out loud
What it accomplishes: Labeling an emotion — "this is RSD, not reality" — activates the prefrontal cortex and starts to slow the amygdala response. This is affect labeling, and it has support in neuroimaging research from UCLA's Social Cognitive Neuroscience Lab.
Say it simply: "That's my RSD talking." You don't need to believe it fully yet. The act of naming it is enough to create a small buffer between the feeling and your reaction. Speak it, don't just think it — vocalization adds a sensory anchor.
Expected outcome: The emotion doesn't disappear, but it becomes something you're observing rather than something that's consuming you.
Step 3 — Use a physical regulation tool immediately
What it accomplishes: RSD is a body event. Your heart rate spikes, your chest tightens, your jaw clenches. A physical tool brings the nervous system down before you try to do anything cognitive.
Box breathing is one of the most effective options: inhale for 4 counts, hold for 4, exhale for 4, hold for 4. Repeat 4–6 times. Cold water on the wrists works. So does a brief walk — 5 minutes is enough to measurably lower cortisol. Pick one tool and practice it when you're calm, so it's automatic when you're not. You can also read more about box breathing and its effect on the nervous system on Lovon's blog.
Common mistake: Reaching for a screen, social media, or a text message during the spike. Seeking reassurance in that state usually makes RSD worse — it confirms the pattern of needing external validation to feel okay.
Step 4 — Talk it through before you act on it
What it accomplishes: RSD episodes push you toward immediate action — sending the message, confronting the person, quitting the job. Talking through what happened creates a delay that almost always produces a better outcome.
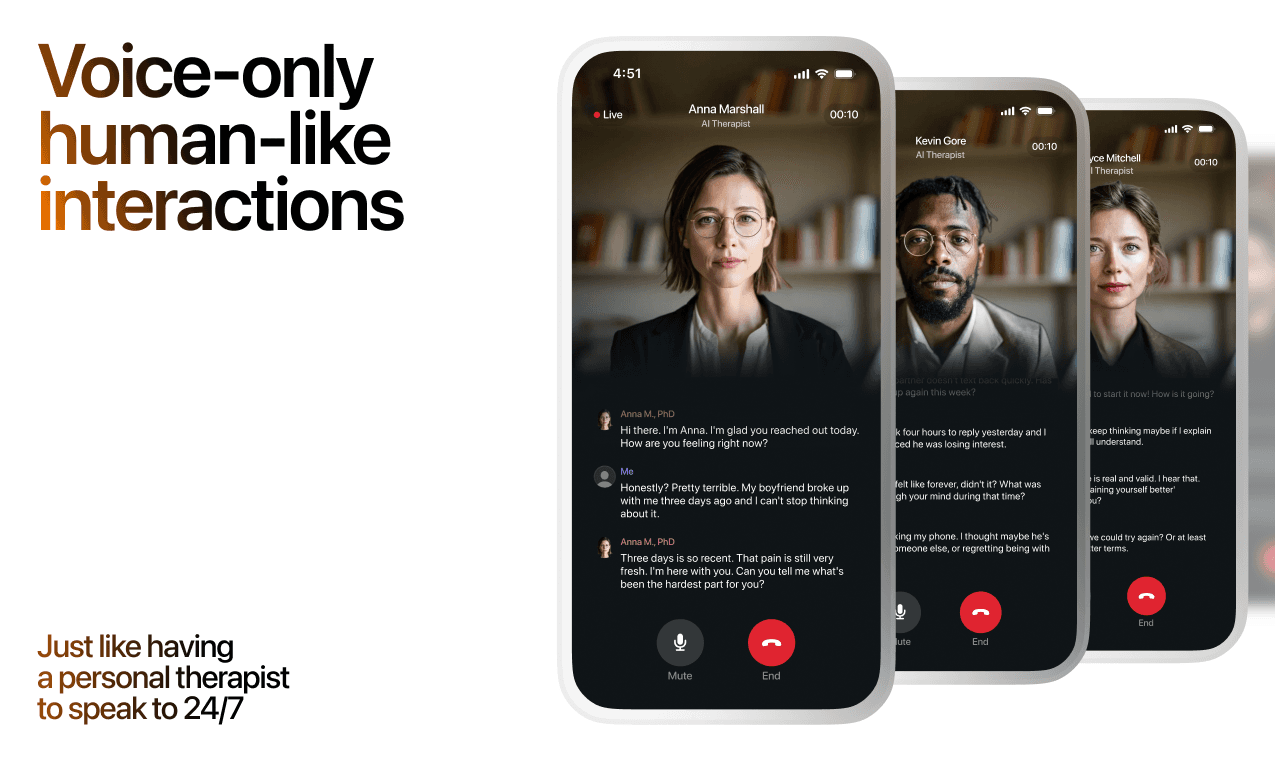
Tell someone you trust what happened and exactly how it felt. If that person isn't available at 11pm when the RSD hits hardest, a voice-based AI tool like Lovon lets you process it in real time — saying what happened out loud, unpacking the emotion, and getting grounded coping questions back. This kind of on-demand voice conversation works well for RSD because it meets you at the moment of the spike, not three days later in a therapy office. The AI therapy for ADHD emotional regulation guide explains how this kind of support fits into a broader ADHD care plan.
Common mistake: Venting to the person who triggered the RSD before you've regulated. This almost always escalates the situation.
Step 5 — Reality-test the perceived rejection
What it accomplishes: Once your nervous system is calmer — usually 20–30 minutes after the initial spike — you can use cognitive restructuring to check whether the perceived rejection was real.
Ask three questions: What is the evidence this rejection actually happened? What's the most neutral explanation for what I observed? What would I tell a close friend who described this same situation to me? Write the answers. The ADHD brain, once calm, is capable of this reasoning — it just can't access it during the flood.
Expected outcome: You'll frequently find the rejection was partial, ambiguous, or entirely imagined. That insight doesn't erase the pain, but it prevents you from taking actions you'd regret.
Step 6 — Identify the underlying fear
What it accomplishes: Every RSD trigger points to a specific core fear — usually "I'm not good enough," "I'll be abandoned," or "I'm too much for people." Knowing your core fear turns a pattern of random emotional eruptions into something you can work on systematically.
Therapy is the most effective route here, specifically trauma-informed CBT or EMDR when the core fear is tied to early experiences. If cost or access is a barrier, the 2026 therapy cost guide breaks down what to expect without insurance and where to find low-cost options.
Common mistake: Skipping this step because the episode is over and you feel okay. RSD doesn't get better without understanding the pattern underneath it.
Step 7 — Build a RSD response plan before the next episode
What it accomplishes: A written plan reduces decision fatigue in the moment. When RSD hits, your working memory (already impaired by ADHD) shrinks further. A physical card or phone note with your 3-step response sequence means you don't have to remember what to do.
Your plan should include: your top trigger category, your physical regulation tool, who you call or what app you open, and your reality-testing questions. Review it every two weeks. Update it when something doesn't work. This is a living document, not a one-time exercise.
Troubleshooting
"I recognize the RSD but I still act on it immediately." The gap between recognition and regulation is a skill, and it takes repetition. Start with lower-stakes triggers — not the ones involving your closest relationships — and practice the pause there first. Build the muscle before the high-stakes moments demand it.
"My RSD lasts hours or days, not minutes." Prolonged episodes often involve a secondary layer: rumination. The initial spike fades, but your brain keeps replaying the event. Rumination in ADHD is tied to working memory loops. Scheduled worry time (a 15-minute daily window to process, then stop) and structured journaling can break the loop. Consistent support from a tool like Lovon between therapy sessions helps too — see the ADHD emotional dysregulation tools guide for a broader toolkit.
"People in my life think I'm overreacting." This is one of the hardest parts of RSD. The emotional intensity is real, even if the triggering event seems minor to others. Sharing the neuroscience — specifically that ADHD involves documented differences in emotional regulation circuitry — helps some people understand. Others won't. Knowing the difference matters.
"My RSD is worst in romantic relationships." Intimate relationships amplify RSD because the stakes feel highest. Anxious attachment and RSD interact in ways that create pursuing, reassurance-seeking, and conflict spirals. The anxious attachment style guide covers this overlap in detail.
"Medication isn't helping my RSD." Stimulants primarily target attention and hyperactivity — they don't reliably reduce RSD. Alpha-2 agonists (guanfacine, clonidine) and MAOIs have shown more specific benefit for emotional dysregulation in ADHD in clinical literature. Talk to your prescriber specifically about RSD, not just attention symptoms.
"I can't tell if this is RSD or something else." RSD can look like bipolar disorder (the intensity), BPD (the relationship patterns), and social anxiety (the avoidance). The distinguishing feature of RSD is the speed of onset and offset — it arrives within seconds of the trigger and is usually gone within hours, not days. A formal ADHD evaluation is the clearest path to a correct diagnosis.
Tools and Resources
- Lovon — voice AI support available anytime for processing RSD episodes in real time; built with input from PhD psychologists and explicit about not replacing clinical care
- Free AI therapist for ADHD adults — Lovon's guide to using AI support specifically for ADHD challenges
- ADDitude Magazine — the most reliable lay publication on ADHD; Dr. Dodson's articles on RSD are the starting point for most people
- CHADD (Children and Adults with ADHD) — provides a therapist finder filtered by ADHD specialty
- A licensed therapist trained in ADHD and emotional dysregulation — the single most effective long-term resource
What to Do Next
Understanding RSD is step one. The next step is building the daily emotional regulation habits that prevent episodes from derailing your life. The ADHD and anxiety overlap guide covers how these two conditions interact — which matters because anxiety and RSD often reinforce each other and need different interventions.
FAQ
What is rejection sensitive dysphoria in ADHD? Rejection sensitive dysphoria is an intense, sudden emotional response — shame, rage, or despair — triggered by real or perceived rejection or criticism. It's a feature of ADHD's emotional dysregulation, not a separate disorder, and it's neurological in origin.
Is RSD the same as anxiety? No. Anxiety builds gradually and centers on future-oriented worry. RSD is instantaneous — it spikes within seconds of a trigger and usually resolves within hours. They can co-occur, but the mechanisms are different.
How do I know if I have rejection sensitive dysphoria? Common signs: avoiding situations where criticism is possible, intense emotional pain from small perceived slights, frequent reassurance-seeking in relationships, and a history of adjusting your behavior to prevent others from being displeased. A formal ADHD evaluation can confirm it.
Does everyone with ADHD have RSD? Not everyone, but estimates from ADDitude Magazine place the figure at close to 99% of adults with ADHD reporting at least some rejection sensitivity. Severity varies widely.
Can RSD be treated? Yes. Emotional regulation therapy (especially trauma-informed CBT), certain medications (alpha-2 agonists in particular), and consistent coping practice all reduce RSD's impact. It rarely disappears entirely, but it becomes manageable.
Is RSD in the DSM? Not as a standalone diagnosis. It falls under emotional dysregulation in ADHD. The term was coined clinically and is widely used by ADHD specialists, but it does not appear as its own entry in the DSM-5 as of 2026.
What triggers RSD the most? The most common triggers in 2026 clinical literature are: perceived criticism from a romantic partner, being left out socially, receiving negative feedback at work, and sensing disappointment from someone the person respects. Anticipatory triggers — avoiding situations to prevent possible rejection — are also extremely common.
How long does an RSD episode last? Most peak within 20–30 minutes. The emotional intensity usually resolves within 2–4 hours. Rumination can extend the experience for days, but that's a secondary process, not the RSD episode itself.
One Last Thing
People with ADHD and RSD often become exceptionally perceptive readers of other people's emotions — because they've had to be. That hypervigilance is exhausting, but it also produces real empathy. The same brain that makes rejection feel unbearable also picks up on subtle pain in others that most people miss entirely. That's not a small thing.
Related Guides
How AI Support Helps You Heal
AI emotional support isn't about replacing human connection — it's about filling the gaps. The moments when you need to talk at 2 AM, when you don't want to burden your friends again, or when you simply need someone to listen without judgment.
Here's what happens in a typical Lovon session:
You share what's on your mind
There's no script, no intake form, no waiting room. You speak or type whatever you're feeling — in your own words, at your own pace.
Lovon validates and explores
Using frameworks from CBT (Cognitive Behavioral Therapy) and motivational interviewing, Lovon acknowledges your feelings first, then gently helps you explore them. No dismissive "just move on" advice.
You build coping skills together
Lovon doesn't just listen — it actively works with you on evidence-based techniques: thought reframing, urge surfing, behavioral experiments, and more.
What a Session with Lovon Looks Like
When to Seek Professional Help
AI support is a valuable tool, but it's not a replacement for professional care. Please consider reaching out to a licensed therapist if you experience any of the following:
- Persistent thoughts of self-harm or suicide
- Inability to perform daily activities (work, eating, sleeping) for more than 2 weeks
- Turning to alcohol or substances to cope
- Intense anger or desire to harm your ex-partner
- Complete emotional numbness that doesn't improve over time
Crisis Resources (US): If you're in immediate danger, call 988 (Suicide & Crisis Lifeline) or text HOME to 741741 (Crisis Text Line). Available 24/7, free, and confidential.
Outside the US? Find a crisis line in your country
Ready to Start?
Your healing journey can begin right now
1 free conversation. No credit card. No judgment. Just a safe space to process what you're going through.
Frequently Asked Questions
Is AI therapy a replacement for a real therapist?
Is my conversation with Lovon AI private?
How is Lovon different from ChatGPT for emotional support?
Can I use Lovon if I'm already seeing a therapist?
Can I try Lovon for free?
About the Author
The Lovon Editorial Team
Mental Health & Wellness Content Team
The Lovon Editorial Team develops mental health and wellness content designed to make psychological concepts accessible and actionable. Our goal is to bridge the gap between clinical research and everyday life - helping you understand why your mind works the way it does and what you can do about it....
Similar Articles
Amygdala and Prefrontal Cortex Connection: Training Emotional Regulation Through Mindfulness
How mindfulness practices reshape neural pathways to strengthen emotional control and reduce reactivity
ADHD Comorbidity with Anxiety and Depression Cycles
Understanding the Complex Interplay Between ADHD and Recurring Mental Health Patterns
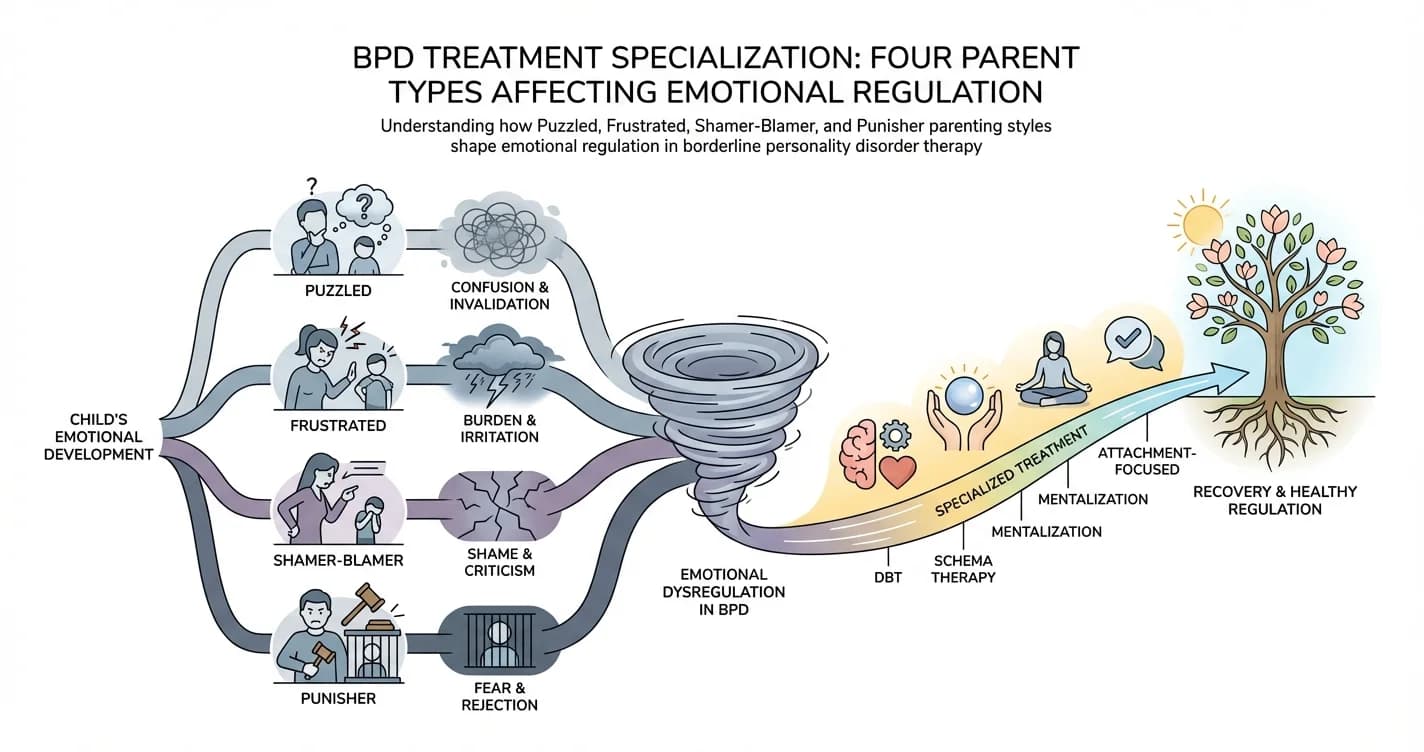
BPD Treatment Specialization: Four Parent Types Affecting Emotional Regulation
For individuals with borderline personality disorder (BPD), emotional regulation difficulties rarely emerge in isolation. Research increasingly suggests that
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. If you are in crisis or think you may have an emergency, call 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room. Outside the US? Find a crisis line in your country.